One of the most interesting (in my opinion) paradox in modern policy debates relates to how Cuba, a very poor country, has been able to generate health outcomes close to the levels observed in rich countries. To be fair, academics have long known that there is only an imperfect relation between material living standards and biological living standards (full disclosure: I am inclined to agree, but with important caveats better discussed in a future post or article, but there is an example). The problem is that Cuba is really an outlier. I mean, according to the WHO statistics, its pretty close to the United States in spite of being far poorer.
In the wake of Castro’s death, I believed it necessary to assess why Cuba is an outlier and creates this apparent paradox. As such, I decided to move some other projects aside for the purposes of understanding Cuban economic history and I have recently finalized the working paper (which I am about to submit) on this paradox (paper here at SSRN).
The working paper, written with physician Gilbert Berdine (a pneumologist from Texas Tech University), makes four key arguments to explain why Cuba is an outlier (that we ought not try to replicate).
The level of health outcomes is overestimated, but the improvements are real
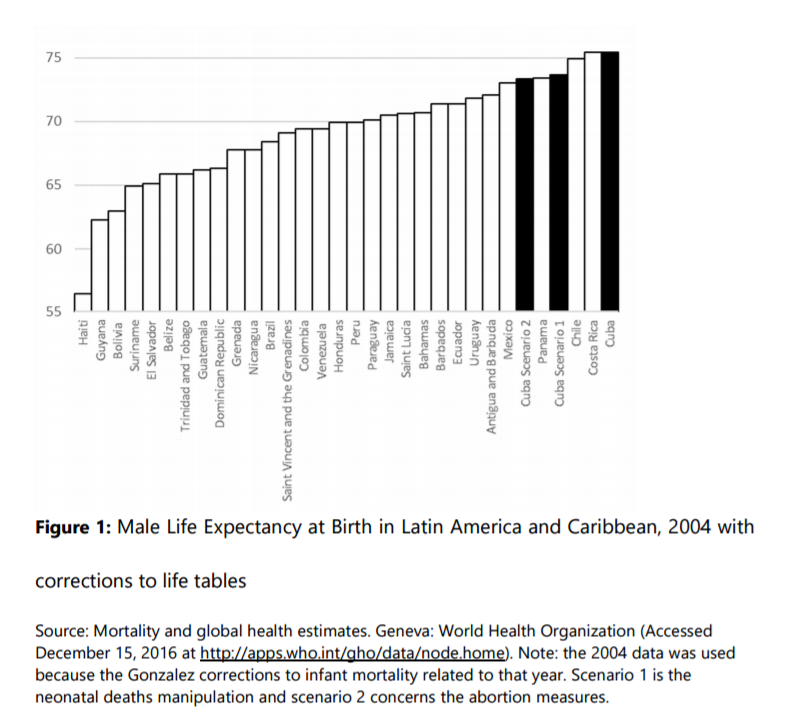
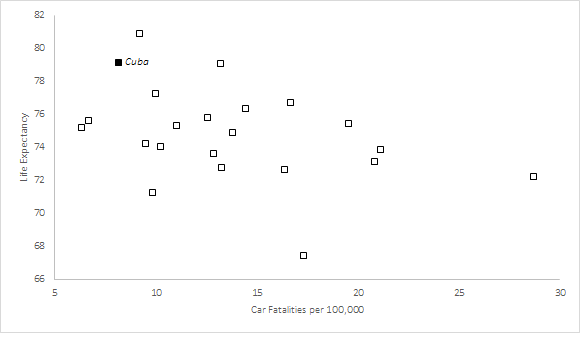
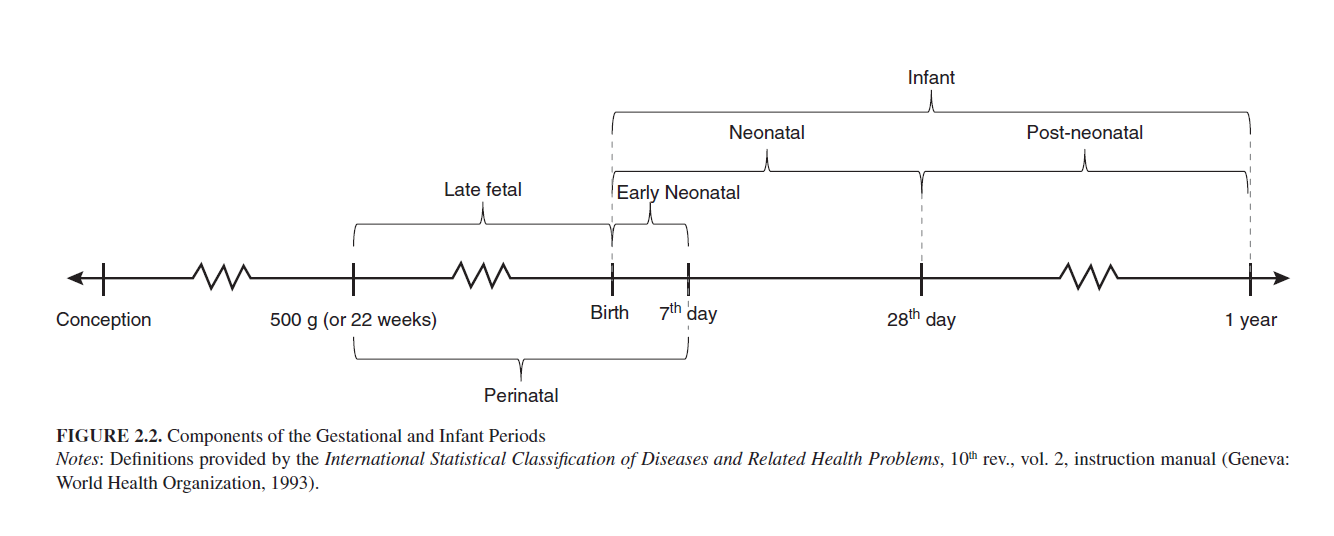
Incentives matter, even in the construction of statistics and this is why we should be skeptical. Indeed, doctors are working under centrally designed targets of infant mortality that they must achieve and there are penalties if the targets are not reached. As such, physicians respond rationally and they use complex stratagems to reduce their reported levels. This includes the re-categorization of early neonatal deaths as late fetal deaths which deflates the infant mortality rate and the pressuring (sometimes coercing) of mothers with risky pregnancies to abort in order to avoid missing their targets. This overstates the level of health outcomes in Cuba since accounting for reclassification of deaths and a hypothetically low proportions of pressured/coerced abortions reduces Cuban life expectancy by close to two years (see figure below). Nonetheless, the improvements in Cuba since 1959 are real and impressive – this cannot be negated.
Health Outcomes Result from Coercive Policy
Many experts believe that we ought to try to achieve the levels of health outcomes generated by Cuba and resist the violations of human rights that are associated with the ruling regime. The problem is that they cannot be separated. It this through the use of coercive policy that the regime is able to allocate more than 10% of its tiny GDP to health care and close to 1% of its population to the task of being a physician. It ought also be mentioned that physicians in Cuba are also mandated to violate patient privacy and report information to the regime. Consequently, Cuban physicians (who are also members of the military) are the first line of internal defense of the regime. The use of extreme coercive measures has the effect of improving health outcomes, but it comes at the price of economic growth. As documented by Werner Troesken, there are always institutional trade-offs in term of health care. Either you adopt policies that promote growth but may hinder the adoption of certain public health measures or you adopt these measures at the price of growth. The difference between the two choices is that economic growth bears fruit in the distant future (i.e. there are palliative health effects of economic growth that take more time to materialize).
Health Outcomes are Accidents of Non-Health Related Policies
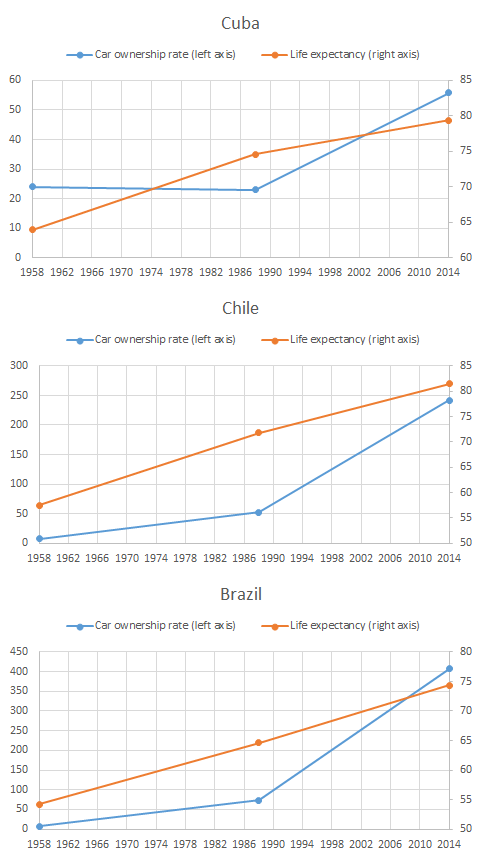
As part of the institutional trade-off that make Cubans poorer, there might be some unintended positive health-effects. Indeed, the rationing of some items does limit the ability of the population to consume items deleterious to their health. The restrictions on car ownership and imports (which have Cuba one of the Latin American countries with the lowest rate of car ownership) also reduces mortality from road accidents which, in countries like Brazil, knock off 0.8 years of life expectancy at birth for men and 0.2 years for women. The policies that generate these outcomes are macroeconomic policies (which impose strict controls on the economy) unrelated to the Cuban health care system. As such, the poverty caused by Cuban institutions may also be helping Cuban live longer.
Human Development is not a Basic Needs Measure
The last point in the paper is that human development requires agency. Since life expectancy at birth is one of the components of the Human Development Indexes (HDI), Cuba fares very well on that front. The problem is that the philosophy between HDIs is that individual must have the ability to exercise agency. It is not a measure of poverty nor a measure of basic needs, it is a measure meant to capture how well can individual can exercise free will: higher incomes buy you some abilities, health provides you the ability to achieve them and education empowers you.
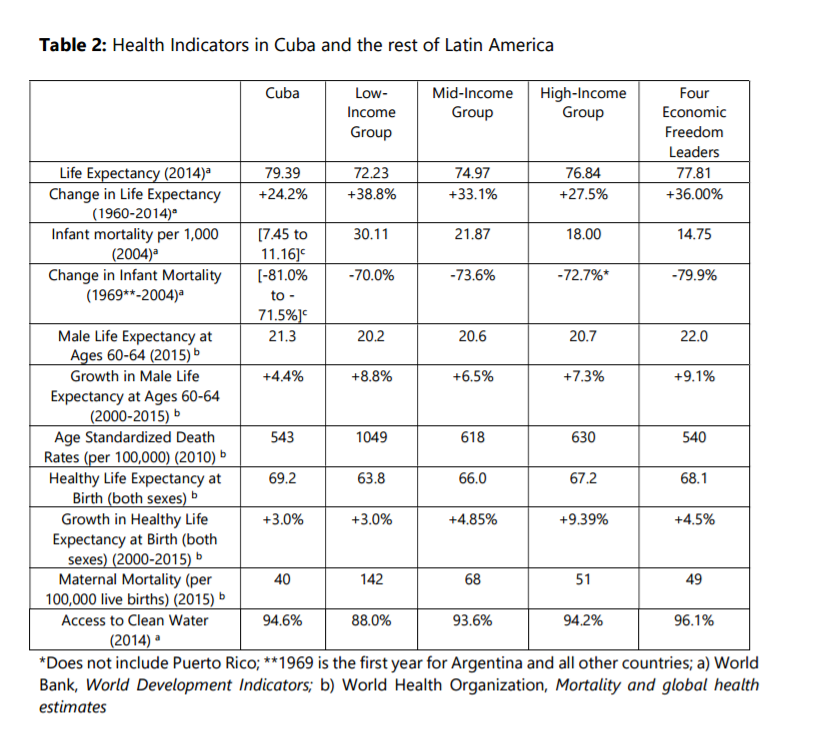
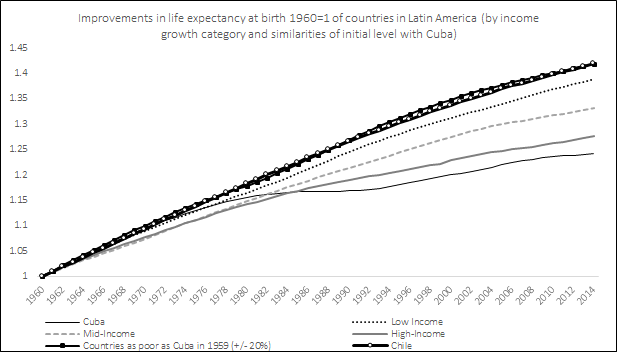
You cannot judge a country with “unfree” institutions with such a measure. You need to compare it with other countries, especially countries where there are fewer legal barriers to human agency. The problem is that within Latin America, it is hard to find such countries, but what happens when we compare with the four leading countries in terms of economic freedom. What happens to them? Well, not only do they often beat Cuba, but they have actually come from further back and as such they have seen much larger improvements that Cuba did.
This is not to say that these countries are to be imitated, but they are marginal improvements relative to Cuba and because they have freer institutions than Cuba, they have been able to generate more “human development” than Cuba did.
Our Conclusion
Our interpretation of Cuban health care provision and health outcomes can be illustrated by an analogy with an orchard. The fruit of positive health outcomes from the “coercive institutional tree” that Cuba has planted can only be picked once, and the tree depletes the soil significantly in terms of human agency and personal freedom. The “human development tree” nurtured in other countries yields more fruit, and it promises to keep yielding fruit in the future. Any praise of Cuba’s health policy should be examined within this broader institutional perspective.

_-_Local_Chips_(cropped).jpg){kind=link}