Freedom through Knowledge: Liberalism, Censorship, and Public Health in Early Planned Parenthood Campaigns (History of Knowledge)
Can Structural Changes Fix the Supreme Court? (Journal of Economic Perspectives)
The Health Care Crucible (The Baffler)
Freedom through Knowledge: Liberalism, Censorship, and Public Health in Early Planned Parenthood Campaigns (History of Knowledge)
Can Structural Changes Fix the Supreme Court? (Journal of Economic Perspectives)
The Health Care Crucible (The Baffler)
It looks to me (as I refresh tracking numbers) that the post office is still reeling after several months of attempted voter suppression. It also looks to me like even though Trump is on his way out, there is no reason to believe that someone just as terrible couldn’t come along at any point in the next 50 years and outdo him.
As far as the USPS goes I think there’s a fairly simple solution that should make most people happy: split the USPS in two: a private for-profit firm that delivers junk mail and competes with UPS and Amazon, and a government agency that handles government business including things like distributing ballots and census surveys.
But the USPS is just one small part of a much larger problem. When the Trump II comes along, he’ll have more powers, including (very likely) a lot more power to mess with the health care sector. There are a lot of reasons I don’t like the idea of more government in health care, but this one should be terrifying to everyone.
Even though I don’t follow the news, it’s somewhat impossible not to know that Bernie Sanders is making a lot of buzz as the possible Democrat candidate for the coming presidential elections. I know: he presents himself as a democratic socialist; he says that some European countries are good examples for the US. I believe that as a Brazilian I have something to say about that.
Bernie Sanders often compares the US with countries like Denmark or Sweeden. I believe there is a fundamental problem with that: the US is a gigantic country with a gigantic population. And a very diverse population at that! Nordic countries are tiny, with a tiny and homogenous population. How about comparing the US and Brazil? The two countries have about the same size and the population is not too different. Besides, Brazil is as culturally diverse as the US. Maybe more!
So here are some things about Brazil that I think people should know. Brazil is by definition a social democracy. That is not written anywhere, but one has only to read our constitution to be aware of that. Brazil’s constitution is very young: it was promulgated in 1988. As so, it reflects more recent political ideas. For example, it basically puts healthcare as a human right that the government has to provide for the population. So, Brazil has (in theory) a free universal healthcare system.
How is healthcare in Brazil in reality? Horrible. Inhumane. Media news are basically the same every week: long waiting lines for the most basic treatments. People dying without care. Few doctors. Overprice. Medication and equipment rooting without use. I don’t think that people in Brazil are different from people in the US. We have the same chromosomes. The difference is in how we deal with the issue. Brazil decided that healthcare is a right and that it should be provided by the government. The result is that we don’t have healthcare.
I believe I know why things are the way they are in Brazil: healthcare is a need. No doubt about that! But there is something really bad when a need is turned into a right. A right means that you have to get it, no matter what. But, really? No matter what? Second, there is something very deceiving when one talks about “free” healthcare. Really? Free?! Doctors have to get paid. Medicine costs money. One can’t possibly be serious when they say “free healthcare”. Finally, I suspect that the Austrian School of economics has something very important to say about the government running the healthcare system. More than anyone else, Friedrich Hayek pointed to how free prices are important for the economy. In a truly free economy, supply and demand interact with prices: high prices mean low supply; low prices mean high supply. This simple mechanism functions as a compass for everyone. However, when the government interferes, the result is inefficiency. Too much medicine is bought and just rots. Or too little, and people die.
I’m not sure how many Bernie supporters read Notes on Liberty. But I really wish some of them would check what happens in Brazil. We tried to have a free universal healthcare system. We tried to have free college. We tried all these things. It didn’t work. I believe that the Austrian School can explain why. I know, it’s a bummer. There is nothing nice about people dying for lack of treatment. However, if you agree with me that this is a problem, I believe I’m in the right position to say that socialism – democratic or not – is not the solution.
I just spent three and a half weeks in Puerto Vallarta, Mexico (summer 2019). Below are some impressions. First things first; I have to give you the severe limits of my field of vision while I was there.
My wife and I stayed in an old-fashioned, 1950s low-rise hotel on the ocean with a pleasant faded kind of glory. (My wife Krishna does not let me go to Mexico by myself, for obvious reasons!) It was very hot throughout so, we did not go out much except that we had to shop for food every day at the mall across a broad avenue. We took taxis to and from the dentist about fifteen times. I always chat with taxi drivers; they gave us the foundation of sociology, I am sure! We spent a little time in the old touristy market district (where we have friendly acquaintances from past visits). We also walked some on Puerto Vallarta’s beautiful and interesting seafront (the “malecon”). I speak Spanish well, I understand everything in the language; I read it with ease. I read the paper a few times; I watched the Spanish language news on television a few times. I read free brochures on this and that.
There is much to like in Mexico, and especially Mexicans. They are low-key, unexcitable, stoical cordial, affable, and eager to help, and not only vis-à-vis this pleasant, well-disposed gringo, myself. Living for a short time in pleasant, clean Puerto Vallarta, it’s difficult to remember that Mexico’s homicide rate is three times the US rate. It takes the occasional sighting of a truckful of the new, nattily dressed National Guard with automatic weapons to jog your memory. (See notes from a previous visit: “Mexicans in Mexico,” 2017, )
Low productivity
My main observation is a repeat from what I recounted the last time I was there (See my “Mexican Underdevelopment: Pop-Sociology.”) It’s about productivity. For most of our stay, there was work going on on a brick path right beneath my windows. It was mind boggling. At one point, there were seven people working on the same two steps, including a master craftsman. They continued by restoring and cleaning a flat brick path. The thought stuck me that,in California, two, or two-and-a-half of the same Mexican workers (the very same guys) would have done the same work in the same time easily. And, yes, I know something about brick laying, both personally (I used to be very poor; now I am moderately poor), and as a customer. I am talking about a more than fifty per cent rise in productivity obtained by simply moving workers into a different environment. Bosses and economic leaders would easily kill for a change of such magnitude!
Of all the guys on the bricklaying and brick cleaning site, only one had a proper power tool, and it was only operational part of the time. The others labored by hand, mostly on their knees. No one had thought of giving them knee-guards. They had not themselves.
Moderate Poverty
The workers told me they were making about US$23 a day, or $115 for a forty-hour week. That’s not bad given that beginning professional positions – that require a university education – in thriving, manufacturing Monterrey are advertised for US$600 a month. Yet, and although most food, housing, gasoline, and health care are all cheaper in Mexico than in the US, this is still not much money on which to rear a family. But, this is also not dire poverty of the kind we used to see, and sometimes still find in India or in Africa. In that part of Mexico, everyone looks healthy, especially the children. Many adults are obese, more or less like in the US. Everyone is well dressed, by the admittedly low standards of central California where I live.
Over-staffing
Here is striking fact: Wherever you go, you find overstaffed shops, restaurants, etc, often very overstaffed. I mean like three shop attendants doing nothing in the middle of the afternoon. There must be a reasonable number of exceptions because my dentist’s office makes good use of its human resources. The same young women who serve as assistants, also act as receptionists. (I know, know, comparative advantage; don’t get me started, this is not the time or place.)
Productivity and Income
Over-staffing and the failure to provide workers with the best tools matter a great deal if you think, as I do, that incomes roughly follow productivity though often with big time lags, and often not in a linear fashion. Although employers sometimes fail to share the product of productivity gains with workers, the fact is that they cannot share gains that have not occurred. Low productivity pretty much guarantees low wages.
Note what I am not saying. The Mexican work ethic is not the problem. The guys who worked in the hot sun of tropical Mexico for eight hours a day don’t need lessons from anyone on that count. Also, those of us who live in California remember well the recession years when the vegetable picking lines remained nearly all-Mexican (with a handful of Filipinos) while poor Anglos lamented the absence of jobs. Now that wages in the field have increased substantially because of a chronic farm labor shortage, still few college students are flooding in, California sky-high rents or not.
Going back to fairly prosperous Puerto Vallarta, where construction is thriving (because of Canadian refugees from the cold, I am told), there is also the mysterious fact of the invisible zealot pounding stakes close to my hotel at 5:30 AM. I am not complaining. I respect this instance of unreasonable industriousness!
Social Structure and Productivity
Mexicans remain poor, the Mexican economy keeps growing but only slowly. This is, at least in part, I think, because Mexicans have normative standards that do not feed high productivity. These standard maintain a permanent social structure that makes increasing productivity difficult. A vicious/virtuous circle is at work. Labor is cheap because of its low productivity. It’s so cheap that, why not hire an additional worker for the same job? The incentive to hire nonchalantly is probably high because of Mexicans’ high connectivity. Mexicans, even in a fairly new city like Puerto Vallarta appear much more interconnected than Californians. (I don’t know much about the East Coast of the US.) There are many more individuals in one’s life there to please by giving their relatives and liege a job than is the case where I live.
Take the lifelong relationship of “compadre” and “comadre” between adults who are usually not kin to each other. The titles denote the link between a man and a woman who are respectively godfather and godmother to the same child. It easily multiplies by two or three beyond actual relatives the circle of individuals to whom one is to some extent obligated. And, it does not end there. Why, there is even a word in Mexican Spanish to denote the relationship of two people who have the same first name! I forgot the word but I was charmed to discover that I was ##### to any number of “Diegos.” I can even imagine situations where someone would succeed in using that tenuous link to extract a small favor from me (with a probable intention to reciprocate).
High Connectivity not a Specific Feature of Mexico, and Over-Staffing
I don’t think this high connectivity is an idiosyncratic feature of Mexican society. I believe rather that something similar prevails in India (that I know a little). It seems to me that high connectivity was visible also, in rural Brittany when I was a child in the forties and fifties. It was largely absent in Paris by contrast where I lived most of the time (Order my book of socio-historical memoirs of that period: I Used to Be French: An Immature Autobiography; avoid the middle person, go through me.). Having obligations to few rather than to many is a salient feature of modernity (that includes also urbanization, small nuclear families, and a search for formal education).
I speculate that Mexicans, even in comparatively modern places like Puerto Vallarta, have a high tolerance for over-staffing because of the large social networks within which they exist. Over-staffing is thus a primary contributor to low productivity. Low productivity keeps many people poor. Poor people need a supportive network more than do the more prosperous. Long and short of it: to break the cycle would require a degree of de-humanization of Mexican society. It’s not inexorable. Mexicans may collectively choose a bearable level of poverty (see life expectancy below) over the destruction of the emotional comfort larger social networks promote.
Not Following in the Footsteps….
It seems to me that a high degree of familiarity with the negative example of American society next door with its low connectivity – in places – may guide them toward such a choice. In point of fact, I have met a strikingly large number of Mexican men who had worked in the US for several years and who had returned home under their own power, by choice, according to their narratives. (I also note with satisfaction that ten years ago, S. Nikiforov and I had evoked precisely that sort of preference in a big article on Mexican immigration: “If Mexicans and Americans could cross the border freely,” in The Independent Review, 14-1: 101-133 [Summer] 2009.)
There is no law of nature that requires the people of less developed countries to retrace all the steps of their predecessors in development. The cellphone shows us that often, they don’t have to: Several African countries have phone landlines only in the center of their major city but 80% of their population has access to a cellphone. Trying to skip stages is the rational thing to do, of course. I would guess it’s most successful when it depends largely on a myriad of individual decisions, as with cellphones. Nevertheless, it seems to work pretty well – for some reason – even with collective decisions regarding health care, specifically.
Perhaps, societies can pick and choose what features of modernity they actually want thanks to a density of available information and a richness in inter-communications that was unimaginable forty years ago. (That was when I was studying underdevelopment with rigorous methods.) I can picture a partial national consensus forming that says, “We don’t need everything the big guys have; a little bit more of this and of that, and we are OK.” If this scenario is realistic, food, schooling, and health care will probably be its dominant themes. The Mexican food situation appears fine (I will consider contradiction on this.). In my subjective judgment, based on its products, on the average, Mexican K-12 is superior to its American public counterpart.
Illness and Health care
One component of socio-economic underdevelopment and also an obstacle to development in its own right used to be widespread illness. The morbidity figures I saw in the seventies about the situation in the fifties were horrifying. Illness also obstructed development indirectly because it destroyed family units through the death of parents or older siblings, even of aunts and uncles who might have provided. This is largely in the past. The present in poor countries is very different, greatly improved from the narrow standpoint of health. And, it turns out, the Mexican health picture, in particular appears fairly bright.
Single Payer Health Care
Something to think about for my conservative friends: Mexico has single payer healthcare for those who want it. It has a pretty poor reputation, it’s true. A private health network subsists side-by-side with it for the prosperous. (I like that.) Yet, yet, the life expectancy of Mexicans is only 2.6 years lower than that of Americans, same as the difference between the US and the Netherlands (WHO 2015, in Wikipedia). Americans live longer than Mexicans in the same proportion as the Dutch live longer than Americans. So, either, it’s possible to get fairly similar results health-wise at much lower cost than do Americans, or health care does not matter all that much, as far as not dying is concerned. (Hate to twist the knife in the conservative wound but the Dutch also spend much less money than Americans on their health care.)
Incidentally, I am well aware that there are non-economic arguments against entrusting what is now 17% of the US GDP to the government, to any government. But, perhaps, conservatives should restrict themselves to combating govt. health care on political and principle grounds alone. (End of digression.)
Where To?
So, where am I going with this, you may fairly ask? I am expressing my doubts that Mexican society – and other less developed societies – will be forced to undergo the dislocating social change that would be required to improve much its (their) productivity, according to the old schemes. I have to stop here, more or less, but it seems to me that Mexico is more likely to improve first its societal-level productivity by having more women join the work force. The preservation of a high existing level of connectivity – with its baked-in child care and food services – would ease, and facilitate such mass social change, of course.
The two Democratic presidential debates were performed against a broad background of consecrated untruths and the debates gave them new life. Mostly, I don’t use the word “lies” because pseudo-facts eventually become facts in the mind of those who hear them repeated many times. And, to lie, you have to know that what you are saying isn’t true. Also, it seems to me that most of the candidates are more like my B- undergraduates than like A students. They lack the criticality to separate the superficially plausible from the true. Or, they don’t care.
So, it’s hard to tell who really believes the untruths below and who just let’s them pass for a variety of reasons, none of which speaks well of their intellectual integrity. There are also some down-and-out lies that none of the candidates has denounced, even ever so softly. Here is a medley of untruths.
Untruths and lies
I begin with a theme that’s not obviously an untruth, just very questionable. Economic inequality is rising in America or, (alt.) it has reached a new high point. I could easily use official data to demonstrate either. I could also – I am confident – use official figures to show that it’s shrinking or at a new low. Why do we care anyway? There may be good reasons. The Dems should give them. Otherwise, it’s the same old politics of envy. Boring!
Women need equal pay for equal work finally. But it’s been the law of the land for about forty years. Any company that does not obey that particular law is asking for a vast class action suit. Where are the class action suits?
What do you call a “half-truth” that’s only 10% true? Continue reading
Around early August 2018, a research paper from the Mercatus Center at George Mason University by Charles Blahous made both the Wall Street Journal and Fox News within two days. It also attracted attention widely in other media. Later, I thought I heard sighs of satisfaction from conservative callers on talk show radio whenever the paper came up.
One figure from the study came and stayed at the surface and was quoted correctly many times (rare occurrence) in the electronic media. The cost of what Senator Sanders proposed with respect to national health care was:
30 trillion US dollars over ten years (actually, 32.6 over thirteen years).
This enormous number elicited pleasure among conservatives because it seemed to underscore the folly of Senator Bernie Sanders’ call for universal healthcare. It meant implicitly, federal, single-payer, government-organized health care. It might be achieved simply by enrolling everyone in Medicare. I thought I could hear snickers of relief among my conservative friends because of the seeming absurdity of the gigantic figure. I believe that’s premature. Large numbers aren’t always all they appear to be.
Let’s divide equally the total estimate over ten years. That’s three trillion dollars per year. It’s also a little more than $10,000 per American man, woman, child, and others, etc.
For the first year of the plan, Sanders’ universal health care amounts to 17.5% of GDP per capita. GDP per capita is a poor but not so bad, really, measure of production. It’s also used to express average gross income. (I think that those who criticize this use of GDP per capita don’t have a substitute to propose that normal human beings understand, or wish to understand.) So it’s 17.5% of GDP/capita. The person who is exactly in the middle of the distribution of American income would have to spend 17.5% of her income on health care, income before taxes and such. That’s a lot of money.
Or, is it?
Let’s imagine economic growth (GDP growth) of 3% per years. It’s optimistic but it’s what conservatives like me think is a realistic target for sustained performance. From 1950 to 1990, GDP per capita growth reached or exceeded 3% for almost all years. It greatly exceeded 3% for several years. I am too lazy to do the arithmetic but I would be bet that the mean annual GDP growth for that forty-year period was well above 3%. So, it’s realistic and probably even modest.
At this 3% growth rate, in the tenth year, the US GDP per capita will be $76.600. At that point, federal universal health care will cost – unless it improves and thus becomes more costly – 13% of GDP per capita. This sounds downright reasonable, especially in view of the rapid aging of the American population.
Now, American conservative enemies of nationalized health care are quick to find instances of dysfunctions of such healthcare delivery systems in other countries. The UK system was the original example and as such, it accumulated mistakes. More recently, we have delighted in Canadian citizens crossing the border for an urgent heart operation their nationalized system could not produce for months: Arrive on Friday evening in a pleasant American resort. Have a good but reasonable dinner. Check in Sat morning. Get the new valve on Monday; back to Canada on Wednesday. At work on the next Monday morning!
The subtext is that many Canadians die because of a shortage of that great free health care: It nice if you can get it, we think. Of course, ragging on the Canadians is both fair and endlessly pleasant. Their unfailing smugness in such matters is like a hunting permit for mental cruelty!
In fact, though, my fellow conservatives don’t seem to make much of an effort to find national health systems that actually work. Sweden has one, Denmark has one; I think Finland has one; I suspect Germany has one. Closer to home, for me, at least, France has one. Now, those who read my blogging know that I am not especially pro-French or pro-France. But I can testify to a fair extent that the French National Healthcare works well. I have used it several times across the past fifty years. I have observed it closely on the occasion of my mother’s slow death.
The French national health system is friendly, almost leisurely, and prompt in giving you appointments including to specialists. It tends to be very thorough to the point of excessive generosity, perhaps. Yes, but you get what you pay for, I can hear you thinking – just like a chronically pessimistic liberal would. Well, actually, Frenchmen live at least three years longer on the average than do American men. And French women live even longer. (About the same as Canadians, incidentally.)
Now, the underlying reasoning is a bit tricky here. I am not stating that French people live longer than Americans because the French national healthcare delivery system is so superior. I am telling you that whatever may be wrong with the French system that escaped my attention is not so bad that it prevents the French from enjoying superior longevity. I don’t want to get here into esoteric considerations of the French lifestyle. And, no, I don’t believe it’s the red wine. The link between drinking red wine daily and cardiac good health is in the same category as Sasquatch: I dearly hope it exists but I am pretty sure it does not. So, I just wish to let you know that I am not crediting French health care out of turn.
The weak side of the French system is that it remunerates doctors rather poorly, from what I hear. I doubt French pediatricians earn $222,000 on the average. (Figure for American pediatricians according to the Wall Street Journal 8/17/18.) But I believe in market processes. France the country has zero trouble finding qualified candidates for its medical schools. (I sure hope none of my current doctors, whom I like without exception, will read this. The wrong pill can so easily happen!)
By the way, I almost forgot to tell you. Total French health care expenditure per person is only about half as high as the American. Rule of thumb: Everything is cheaper in the US than in other developed countries, except health care.
And then, closer to home, there is a government health program that covers (incompletely) about 55 million Americans. It’s not really “universal” even for the age group it targets because one must have contributed to benefit. (Same in France, by the way, at least in principle.) It’s universal in the sense that everyone over 65 who has contributed qualifies. It’s not a charity endeavor. Medicare often slips the minds of critical American conservatives, I suspect, I am guessing, because there are few complaints about it.
That’s unlike the case for another federal health program, for example the Veterans’, which is scandal-ridden and badly run. It’s also unlike Medicaid, which has the reputation of being rife with financial abuse. It’s unlike the federally run Indian Health Service that is on the verge of being closed for systemic incompetence.
I suspect Medicare works well because of a large number of watchful beneficiaries who belong to the age group in which people vote a great deal. My wife and I are both on Medicare. We wish it would cover us 100%, although we are both conservatives, of course! Other than that, we have no complaints at all.
Sorry for the seeming betrayal, fellow conservatives! Is this a call for universal federal health care in America? It’s not, for two reasons. First, every country with a good national health system also has an excellent national civil service, France, in particular. I have no confidence, less than ever in 2018, that the US can achieve the level of civil service quality required. (Less in 2018 because of impressive evidence of corruption in the FBI and in the Justice Department, after the Internal Revenue Service).
Secondly, when small government conservatives (a redundancy, I know) attempt to promote their ideas for good government primarily on the basis of practical considerations, they almost always fail. Ours is a political and a moral posture. We must first present our preferences accordingly rather than appeal to practicality. We should not adopt a system of health delivery that will, in ten years, attribute the management of 13% of our national income to the federal government because it’s not infinitely trustworthy. We cannot encourage the creation of a huge category of new federal serfs (especially of well-paid serfs) who are likely forever to constitute a pro-government party. We cannot, however indirectly, give the government most removed from us, a right of life and death without due process.
That simple. Arguing this position looks like heavy lifting, I know, but look at the alternative.
PS I like George Mason University, a high ranking institution of higher learning that gives a rare home to conservative American scholars, and I like its Mercatus Center that keeps producing high-level research that is also practical.
This is going to be a short post to argue that pundits (and some economists) need to stop quoting life expectancy figures to argue for/against a particular health care system. This belief is best exemplified in a recent paper in the Journal of the American Medical Association where Papanicolas et al. (2018) point out that the United States “spent nearly twice as much as 10 high-income countries (…) and performed less well on many population health outcomes”. While the authors make good points about administrative costs, they point out that the US has a low level of life expectancy.
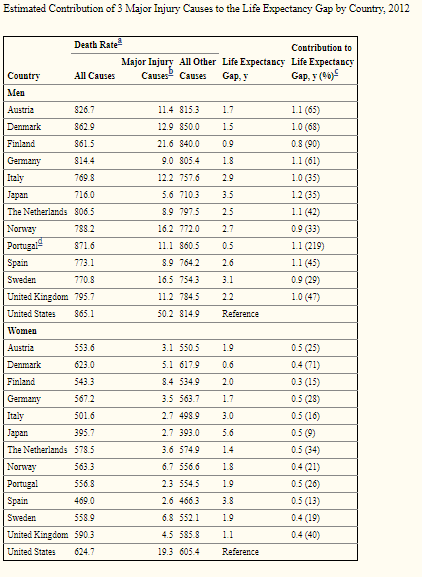
Sure, that is actually true – but Americans tend to die in greater proportions from homicides, drug overdoses and car accidents (Americans drive more than Europeans) than in other rich countries. While these factors of mortality are tragic (except car accidents since Americans seem to prefer the benefits of mobility to the safety of not driving), they are in no way related to the efficiency of health care provision. How much of a deal are these in explaining differences with other industrialized countries? A pretty big deal. For example, these three factors alone account for 64% of the male life expectancy gap between Austria and the United States (see table reproduced below). For women, 26% of the gap between Austria and the United States is explained by these three factors.
The study I cite here only includes three factors. If you add in other factors like drownings among youths (Americans tend to have more drownings than several industrialized countries) which is a result of the fact that Americans are richer and can afford pools (while Europeans tend not to), then you keep explaining away the difference. This is not to say that American health care is great. However, this says that American health care is not as bad as life expectancy outcomes suggest.
In debates over health care reform in the US, it is frequent for Canada’s name to pop up in order to signal that Canada is spending much less of its GDP to health care and seems to generate relatively comparable outcomes. I disagree.
Its not that the system presently in place in the US is so great, its that the measure of resources expended on each system is really bad. In fact, its a matter of simple economics. Imagine two areas (1 and 2), the first has single-payer health care, the other has fully-private health care.
In area 2, prices ration access to health care so that people eschew visits to the emergency room as a result of a scraped elbow. In area 1, free access means no rationing through price and more services are consumed. However, to avoid overspending, the government of area 1 has waiting lists or other rationing schemes. In area 2, which I have presented as an ideal free market for the sake of conversation, whatever people expend can be divided over GDP and we get an accurate portrait of “costs”. However, in area 1, costs are borne differently – through taxes and through waiting times. As such, comparing what is spent in area 1 to what is spent in area 2 is a flawed comparison.
So when we say that Canada spends 10.7% of GDP on health care (2013 numbers) versus 17.1% of GDP in the US, is it a viable comparison? Not really. In 2008, the Canadian Medical Association produced a study evaluating the cost of waiting times for four key procedures : total joint replacement surgery, cataract surgery, coronary artery bypass
graft (CABG) and MRI scans. These procedures are by no means exhaustive and they concern only “excessive” waiting times (rather than the whole waiting times or at least the difference with the United States). However, the CMA found that, for the 2007 (the year they studied), the cost of waiting was equal to 14.8$ billion (CAD). Given the size of the economy back in 2007, this represented 1.3% of GDP. Again, I must emphasize that this is not an exhaustive measure of the cost of waiting times. However, it does bring Canada closer to the United States in terms of the “true cost” of health care. Any estimate that would include other wait times would increase that proportion.
I know that policy experts are aware of that, but it is so frequent to see comparisons based on spending to GDP in order to argue for X and Y policy as being relatively cheap. I just thought it was necessary to remind some people (those who decide to read me) that prudence is mandatory here.
This post is meant to help my non-economist friends think more clearly about how we pay for health care. I’ll talk about markets, but the truth is that the American system is built of deeply bastardized markets. If our car markets worked like our health markets, most of us would walk to work. I’m trying to focus on the essential logic of the situation which is going to sound Utopian because Congress isn’t going to give us any sort of logical policy any time soon. But we aren’t going to get a logical solution until we as voters understand the logic of health care finance.
I’ve got a few big points to make:
(This post is longer than I’d like, so thanks for your patience!)
I’ve said it before, and I’ll say it again: we don’t have to ruin markets to do charity.
The essence of markets is that they aggregate knowledge about the relative costs and benefits of different goods based on the preferences of the real people involved in producing and consuming those goods.
The demand side of markets provide information by giving you (as a consumer) a choice between more of something you like and more money to spend on other stuff. On the supply side they give you (as a supplier–probably of your own labor) the choice between providing more of what people are willing to pay for or having less money to buy the stuff you want. Markets crowdsource cost-benefit analysis.
Prices also give suppliers an incentive to produce things that consumers want while trying to save resources (i.e. cut costs). In other words, a price is a signal wrapped up in an incentive.
So what about fairness? The bad news is that markets are a system of “from each according to their ability, to each according to how much other people are willing to pay for the product of their ability.” (Not very catchy!) It’s mostly fair for most of us, but doesn’t do much good for people who are just unlucky (e.g. kids born with genetic defects). Here’s the good news: we can use charity alongside markets.
We can debate how much role government should play in charity some other time. For now, let’s whole-ass one thing instead of half-assing two things. We have to appreciate that interfering with markets interferes with the ability of those markets to function as sources of reliable information. It doesn’t matter how good our intentions are, we face a trade off here… unless we do something to establish a functioning charity system parallel to the health care finance system.
Anecdotes about the merits of a single-payer health care system are powerful because they shed light on the biggest benefit to such a system: individual convenience.
Part of the appeal has to do with the general screwiness of the American system. It’s a cathedral built of band-aids. But even in an idealized market system, a single-payer system has the advantage of not making me go through the work of evaluating which plan best suits my needs.
A single-payer system is, from an individual perspective, about as ideal as having your parents pay for it. But we don’t really want our parents buying our stuff for us.
Single payer system sacrifice the informational value of markets (probably even more so than America’s current system of quasi-price controls). Innovation would be harder as long as new treatments had to be approved by risk-averse bureaucrats (and again, we already face a version of this with Medicare billing codes and insurance companies).
Essentially, a single payer system creates a common pool problem: each of us gets the individual benefit of being able to be lazy. But then we’re left trusting bureaucrats, special interest groups, and think tanks to keep an eye on things. It could be an improvement over the current American system, but that’s like saying amputation is better than gangrene.
Consider two alternatives. In scenario A you start with $150, flip a coin, and if it comes up tails you lose $100. In scenario B you get $90. The expected value of A is $100, but most of us would still prefer the sure thing.
Here’s how insurance works: You start with $150, give $60 to the insurance company, then flip the coin. If it comes up tails, you lose $100, but the insurance company gives you back $40. You’ve just gotten the sure thing. And by taking on thousands of these bets the insurance company is able to make enough money to pay their employees.
But here’s the thing: the premium they charge is fundamentally tied to that expected value. Change the odds, or the costs (i.e. the claims they have to pay for) and you’ll change the premium.
(BTW, Tim Harford did a nice ~8 minute podcast episode on insurance that’s worth checking out.)
Pre-existing conditions are the equivalent of changing our thought experiment to a 100% chance of flipping tails. No amount of risk sharing that will get you to the $90 outcome you want. You can’t insure your car after you’ve been in an accident and you can’t insure a person against a loss they’ve already realized. If you’re Bill Gates, that’s no big deal, but for many people, this might mean depending on charity. That’s a bummer, but wishful thinking can’t undo that.
If we insist that insurance companies cover pre-existing conditions* the result can only be higher premiums. This is nice for people with these pre-existing conditions, but not so great for (currently) healthy poor people. Again, charity matters needs to be part of the debate, but it needs to be parallel to insurance markets.
Covering more contingencies also affects premiums. The more things a policy covers, the higher the expected cost, and therefore the higher the premium. We each have to decide what things are worth insuring and what risks we’re willing to face ourselves. Politics might not be the best way to navigate those choices.
Actuaries think about the cost of insuring as a marginal cost. In other words, they know that the odds that you spend $100 in a year are much higher than the odds that you spend $1000. So the cost of insuring the first dollar of coverage is much higher than the cost of insuring the 5000th dollar. This is why high deductible plans are so much cheaper… they only pay out in the unlikely situation where something catastrophically bad happens to you. This is exactly why most of us want insurance. We aren’t afraid of the cost of band-aids and aspirin, we’re afraid of the cost of cancer treatment.
For those of us firmly in the middle class, what we really need is a high-deductible plan plus some money in the bank to cover routine care and smaller emergencies. (Personally, my version of this is a credit card.) Such a plan has the added benefit of encouraging us to be more cost conscious.
A big problem with our current system is that it’s set up like an all-you-can-eat buffet. You pay to get in (your premiums) but once you’re in the hospital, any expenses are the insurance company’s problem (read: everyone else on your health plan). The logic here is the same as with pollution. When I drive my car I get the benefits of a quick and comfortable commute but I also suffer a little bit more pollution. But I don’t have incentive to think about how that pollution affects you so I pollute more than would be ideal. Multiply that by millions of people and we can end up with smog.
If I were trying to put together a politically palatable alternative to our current system, I’d have an individual mandate with insurance vouchers for the poor (it’s not very libertarian, and it’s far from my Utopian ideal, but I think it would be a huge improvement over what we’ve got now). I would also expand the role of market competition by encouraging high deductibles plus flexible health savings accounts.
Reality is complicated, but I’m trying to get at the fundamental logic here. We don’t have a properly functioning market system. To get there we need competition, transparency, and a populace with the mental tools and mathematical literacy necessary to understand what their insurance can and can’t do. That’s a tall order, but it doesn’t mean we shouldn’t keep trying to move in that direction.
To have a fruitful debate we need to understand what we want from our healthcare system: help for the poor (charity), convenience, and efficiency from an individual and social perspective. By trying to lump all these things together we muddy the waters and make it harder to understand one another.
*I don’t know what the deal is with the idea that the AHCA will treat rape as a pre-existing condition. Some webpages give a bunch of random tweets as evidence of this, and others call bullshit. Let’s just leave it at this: in a competitive market this would be considered terrible marketing and savvy companies wouldn’t do it. The lesson then is to keep calling companies on bad marketing, and avoid protecting politically powerful companies from market competition.
One of the most interesting (in my opinion) paradox in modern policy debates relates to how Cuba, a very poor country, has been able to generate health outcomes close to the levels observed in rich countries. To be fair, academics have long known that there is only an imperfect relation between material living standards and biological living standards (full disclosure: I am inclined to agree, but with important caveats better discussed in a future post or article, but there is an example). The problem is that Cuba is really an outlier. I mean, according to the WHO statistics, its pretty close to the United States in spite of being far poorer.
In the wake of Castro’s death, I believed it necessary to assess why Cuba is an outlier and creates this apparent paradox. As such, I decided to move some other projects aside for the purposes of understanding Cuban economic history and I have recently finalized the working paper (which I am about to submit) on this paradox (paper here at SSRN).
The working paper, written with physician Gilbert Berdine (a pneumologist from Texas Tech University), makes four key arguments to explain why Cuba is an outlier (that we ought not try to replicate).
The level of health outcomes is overestimated, but the improvements are real
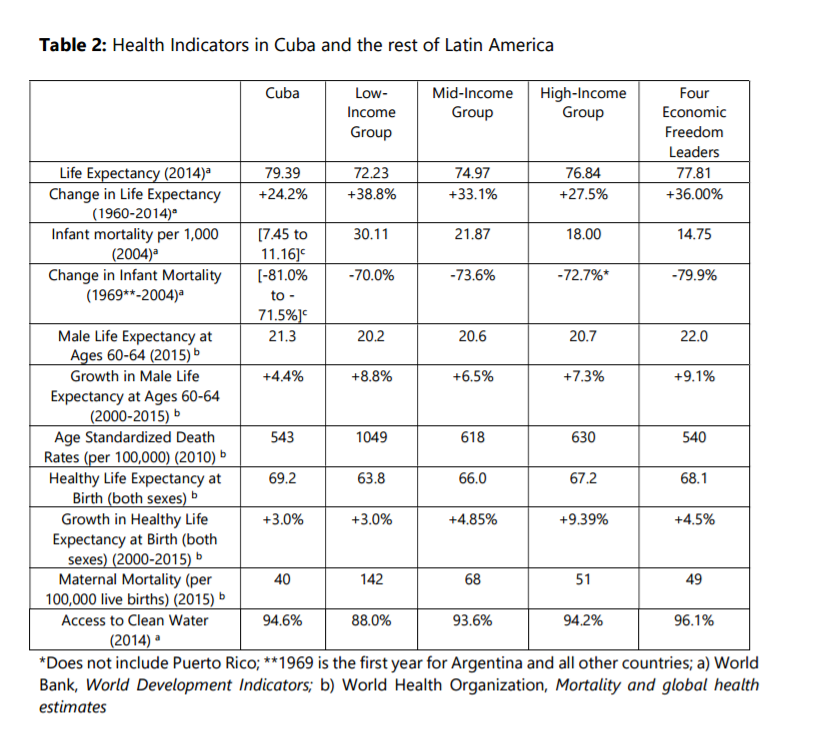
Incentives matter, even in the construction of statistics and this is why we should be skeptical. Indeed, doctors are working under centrally designed targets of infant mortality that they must achieve and there are penalties if the targets are not reached. As such, physicians respond rationally and they use complex stratagems to reduce their reported levels. This includes the re-categorization of early neonatal deaths as late fetal deaths which deflates the infant mortality rate and the pressuring (sometimes coercing) of mothers with risky pregnancies to abort in order to avoid missing their targets. This overstates the level of health outcomes in Cuba since accounting for reclassification of deaths and a hypothetically low proportions of pressured/coerced abortions reduces Cuban life expectancy by close to two years (see figure below). Nonetheless, the improvements in Cuba since 1959 are real and impressive – this cannot be negated.
Health Outcomes Result from Coercive Policy
Many experts believe that we ought to try to achieve the levels of health outcomes generated by Cuba and resist the violations of human rights that are associated with the ruling regime. The problem is that they cannot be separated. It this through the use of coercive policy that the regime is able to allocate more than 10% of its tiny GDP to health care and close to 1% of its population to the task of being a physician. It ought also be mentioned that physicians in Cuba are also mandated to violate patient privacy and report information to the regime. Consequently, Cuban physicians (who are also members of the military) are the first line of internal defense of the regime. The use of extreme coercive measures has the effect of improving health outcomes, but it comes at the price of economic growth. As documented by Werner Troesken, there are always institutional trade-offs in term of health care. Either you adopt policies that promote growth but may hinder the adoption of certain public health measures or you adopt these measures at the price of growth. The difference between the two choices is that economic growth bears fruit in the distant future (i.e. there are palliative health effects of economic growth that take more time to materialize).
Health Outcomes are Accidents of Non-Health Related Policies
As part of the institutional trade-off that make Cubans poorer, there might be some unintended positive health-effects. Indeed, the rationing of some items does limit the ability of the population to consume items deleterious to their health. The restrictions on car ownership and imports (which have Cuba one of the Latin American countries with the lowest rate of car ownership) also reduces mortality from road accidents which, in countries like Brazil, knock off 0.8 years of life expectancy at birth for men and 0.2 years for women. The policies that generate these outcomes are macroeconomic policies (which impose strict controls on the economy) unrelated to the Cuban health care system. As such, the poverty caused by Cuban institutions may also be helping Cuban live longer.
Human Development is not a Basic Needs Measure
The last point in the paper is that human development requires agency. Since life expectancy at birth is one of the components of the Human Development Indexes (HDI), Cuba fares very well on that front. The problem is that the philosophy between HDIs is that individual must have the ability to exercise agency. It is not a measure of poverty nor a measure of basic needs, it is a measure meant to capture how well can individual can exercise free will: higher incomes buy you some abilities, health provides you the ability to achieve them and education empowers you.
You cannot judge a country with “unfree” institutions with such a measure. You need to compare it with other countries, especially countries where there are fewer legal barriers to human agency. The problem is that within Latin America, it is hard to find such countries, but what happens when we compare with the four leading countries in terms of economic freedom. What happens to them? Well, not only do they often beat Cuba, but they have actually come from further back and as such they have seen much larger improvements that Cuba did.
This is not to say that these countries are to be imitated, but they are marginal improvements relative to Cuba and because they have freer institutions than Cuba, they have been able to generate more “human development” than Cuba did.
Our Conclusion
Our interpretation of Cuban health care provision and health outcomes can be illustrated by an analogy with an orchard. The fruit of positive health outcomes from the “coercive institutional tree” that Cuba has planted can only be picked once, and the tree depletes the soil significantly in terms of human agency and personal freedom. The “human development tree” nurtured in other countries yields more fruit, and it promises to keep yielding fruit in the future. Any praise of Cuba’s health policy should be examined within this broader institutional perspective.
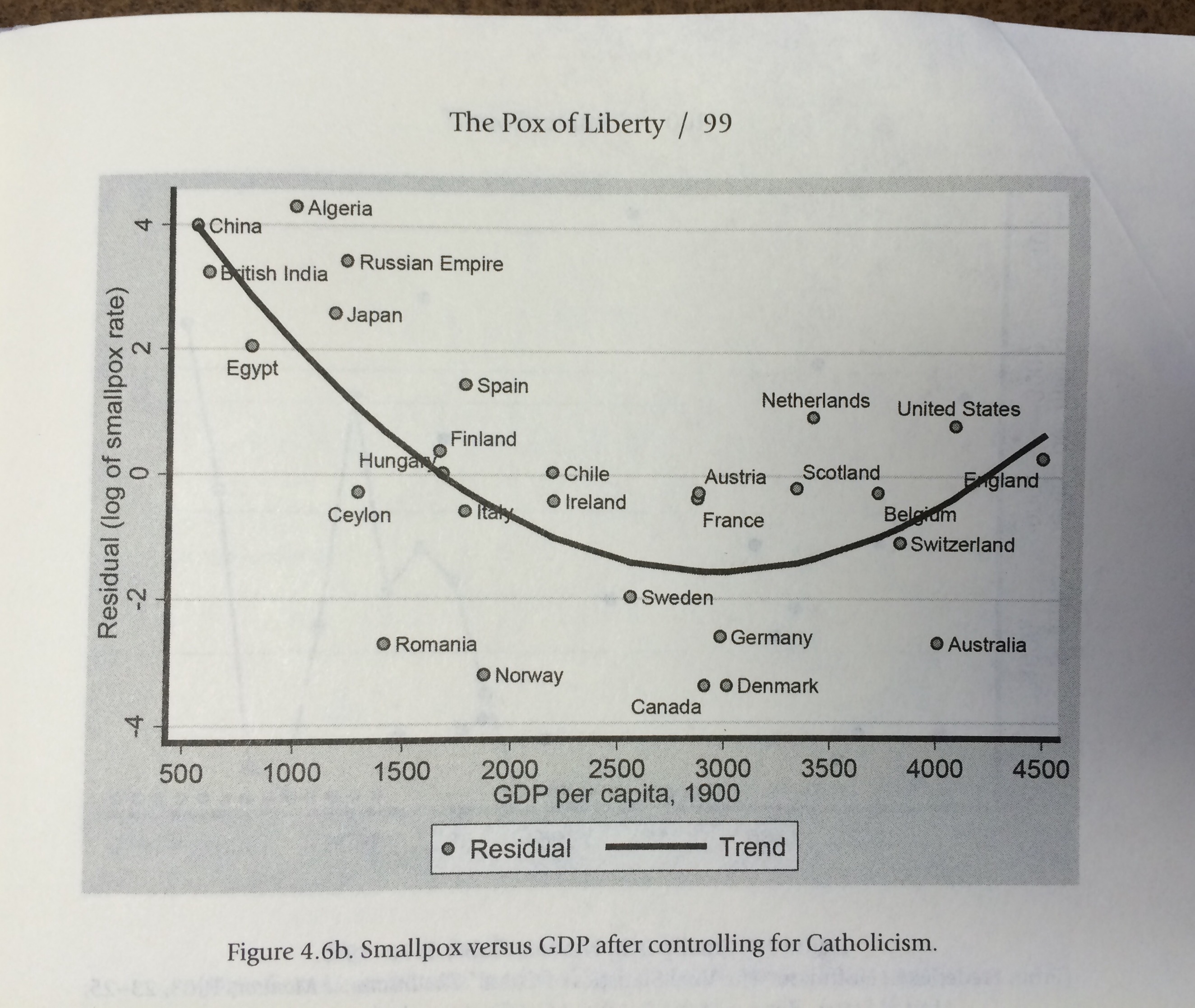
A few weeks ago, I finished reading the Pox of Liberty authored by Werner Troesken. Although I know some of his co-authors personally (notably the always helpful Nicola Tynan whose work on water economics needs to be read by everyone serious in the field of economic history – see her work on London here), I never met Troesken. Nonetheless, I am what you could call a “big fan” in the sense that I get a tingling feeling in my brain when I start reading his stuff. This is because Troesken’s work is always original. For example, his work on the economic history of public utilities (gas and electricity) in the United States is probably one of the most straightforward application of industrial organization to historical questions and, in the process, it kills many historical myths regarding public utilities. The Pox of Liberty is no exception and it should be read (at the risk of become a fan of Troesken like I am) as a treatise on the political economy of public health.
Very often, it will be pointed out that public health measures are public goods that government should provide lest it be “underprovided” if left to private actors. After all, it is rare to hear of individuals who voluntarily quarantined themselves upon learning they were sick. As a result, the “public economics” argument is that the government should mandate certain measures (mandatory vaccination and quarantine) that will reduce infectious diseases. Normally, the story would end there. And to be sure, there is a lot of evidence that mild coercive measures do reduce some forms of mortality (mandatory vaccination and quarantine). The more intense the policies, the larger the positive effects on health outcomes. For example, taxes on cigarettes do reduce consumption of cigarettes and thus, secondhand smoke. In fact, even extreme coercive measures like smoking bans seem to yield improvements in terms of public health (another example is that of Cuba which I discussed on this blog).
However, Troesken’s contribution is to tell us that the story does not end there. In a way, the “public economics” story is incomplete. The institutions that are best able to deploy such levels of coercion are generally also the institutions that are unable to restrain political meddling in economic affairs. Governments that are able to easily deploy coercive measures are governments that tend to be less constrained and they can fall prey to rent-seeking and regulatory capture. They will also tend to disregard property rights and economic freedom. This implies slower rates of economic growth. As a result, there is a trade-off that exists: either you get fast economic growth with higher rates of certain infectious diseases or you get slow economic growth with lower rates of certain infectious diseases (Troesken concentrates mostly on smallpox and yellow fever). The graphic below illustrates this point of Troesken. Countries like Germany – with its strong centralizing Prussian tradition – were able to generate very low levels of deaths from infectious diseases. But, they were poorer than the United States. The latter country had a constitutional framework that limited the ability of local and state governments to adopt even mild measures like mandatory vaccination. Thus, that meant higher mortality levels but the same constitutional constraints permitted economic growth and thus the higher level of living standards enjoyed by Americans relative to the Germans.
But Troesken’s story does not end there. Economic growth has some palliative health effects (in part the McKeown hypothesis*) whereby we have a better food supply and access to better housing or less demanding jobs. However, in the long-run economic growth means that new sectors of activity can emerge. For example, as we grow richer, we can probably expend more resources on drugs research to extend life expectancy. We can also have access to more medical care in general. These fruits take some time to materialize as they grow more slowly. Nonetheless, they do form a palliative effect that contributes to health improvements.
However, there is an analogy that allows us to see why these palliative effects are important in any political economy of public health provision. This analogy relates to forestry. The health outcomes fruits from a “coercive institutional tree” can only be picked once. Once they are picked, the tree will yield no more fruits. However, the yield from that single harvest is considerable. In comparison, the “economic growth tree” yields fewer and smaller fruits, but it keeps yielding fruits. It never stops yielding fruits. In the long-run, that tree outperforms the other tree. The problem is that you cannot have both trees. If you chose one, you can’t have the other.
In this light, public health issues become incredibly harder to decipher and understand. However, we can see a much richer wealth of information under this light. In writing the Pox of Liberty, Troesken is enlightening and anyone doing health economics should read (and absorb his work) as it is the first comprehensive treatise of the political economy of public health.
* I should note that I think that the McKeown hypothesis is often unfairly lambasted and although I have some reservations myself, it can be adapted to fit within a wider theoretical approach regarding institutions – like Troesken does.
As part of my series of blog post reconsidering health outcomes in Cuba, I argued that other countries were able to generate substantial improvements in life expectancy even if Cuba is at the top. Then I pointed out that non-health related measures made Cubans so poor as to create a paradoxical outcome of depressing mortality (Cubans don’t have cars, they don’t get in car accidents, life expectancy is higher which is not an indicator of health care performance). Today, I move to the hardest topic to obtain information on: refugees.
I have spent the last few weeks trying to understand how the Cuban refugees are counted in the life tables. After scouring the website of the World Health Organization and the archives of Statistics Canada during my winter break, I could not find the answer. And it matters. A lot.
To be clear, a life table shows the probability that an individual of age X will die by age X+1 (known as Qx). With a life table, you will obtain age-specific death rates(known as Mx), life expectancy at different points and life expectancy at birth (Lx)(Where x is age). Basically, this is the most important tool a demographer can possess. Without something like that, its hard to say anything meaningful in terms of demographic comparison (although not impossible).The most common method of building such a table is known as a “static” method where we either compare the population structure by age at a single point in time or where we evaluate the age of deaths (which we can compare with the number of persons of each group alive – Ax). The problem with such methods is that static life tables need to be frequently updated because we are assuming stable age structure.
When there is important migration, Qx becomes is not “mortality” but merely the chance of exiting the population either by death of migration. When there are important waves of migration (in or out), one must account for age of the entering/departing population to arrive at a proper estimates of “exits” from the population at each age point that separate exits by deaths or exits (entries) by migration.
As a result, migration – especially if large – creates two problems in life tables. It changes the age structure of the population and so, the table must be frequently updated in order to get Ax right. It also changes the structure of mortality (exits). (However, this is only a problem if the age structure of migrants is different from the age structure of the overall population).
Since 2005, the annual number of migrants from Cuba to the United States has fluctuated between 10,000 and 60,000. This means that, on an annual basis, 0.1% to 0.5% of Cuba’s population is leaving the country. This is not a negligible flow (in the past, the flow was much larger – sometimes reaching north of 1% of the population). Thus, the issue would matter to the estimation of life tables. The problem is we do not know how Cuba has accounted for migration on both mortality and the reference populations! More importantly, we do not know how those who die during migration are measured.
Eventually, Ax will be adjusted through census-based updates (so there will only be a drift between censuses). However, if the Cuban government counts all the migrants as alive as they arrive in a foreign country as if none died along the way, it is underestimating the number of deaths. Basically, when the deaths of refugees and emigrants are not adequately factored into survival schedules, mortality schedules are be biased downward (especially between censuses as a result of poor denominator) and life expectancy would be accordingly biased upward.
Now, I am willing to reconsider my opinion on this particular point if someone indicates some study that has escaped my gaze (my Spanish is very, to put it euphemistically, poor). However, when I am able to find such information for other Latin American countries like Chile or Costa Rica and not for Cuba, I am skeptical of the value of the health statistics that people cite.
The other parts of How Well Has Cuba Managed To Improve Health Outcomes?
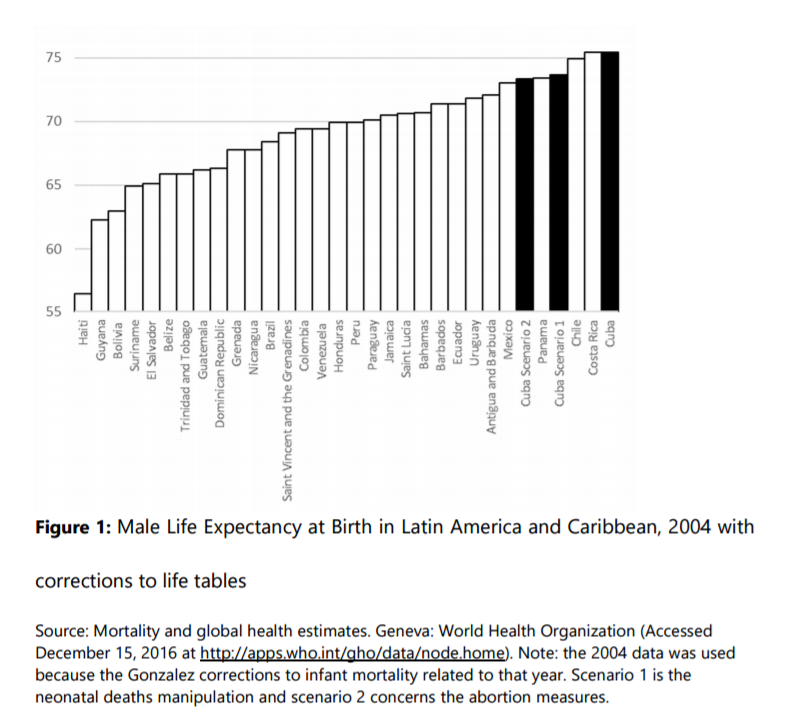
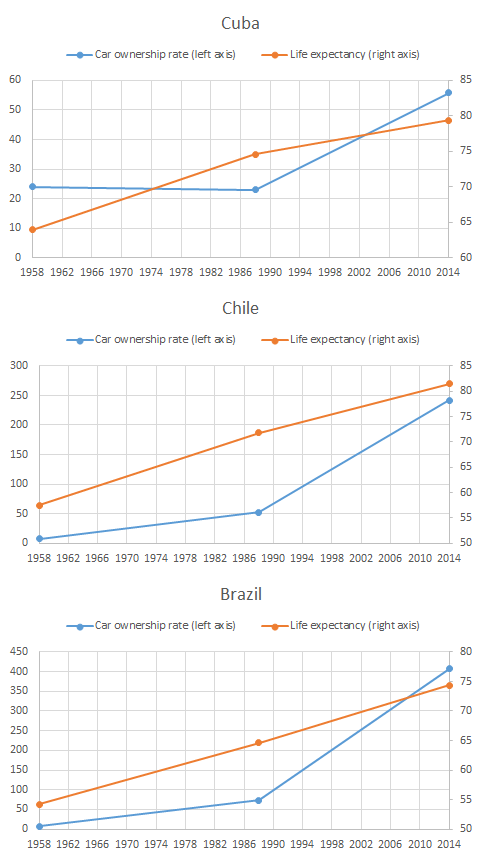
In a recent post, I pointed out that life expectancy in Cuba was high largely as a result of really low rates of car ownerships. Fewer cars, fewer road accidents, higher life expectancy. As I pointed out using a paper published in Demography, road fatalities reduced life expectancy by somewhere between 0.2 and 0.8 years in Brazil (a country with a car ownership rate of roughly 400 per 1,000 persons). Obviously, road fatalities have very little to do with health care. Praising high life expectancy in Cuba as the outcome Castrist healthcare is incorrect, since the culprit seems to be the fact that Cubans just don’t own cars (only 55 per 1,000). But that was a level argument – i.e. the level is off.
It was not a trend argument. The rapid increase in life expectancy is undeniable, so my argument about level won’t affect the claim that Cubans saw their life expectancy increase under Castro.
I say “wait just a second”.
Cuba is quite unique with regards to car ownership. In 1958, it had the second highest rate of car ownership of all Latin America. However, while the rate went up in all of Latin America between 1958 and 1988, it went down in Cuba. During that period, life expectancy went up in all countries while there were substantial increases in car ownership (which would, all things being equal, slow down life expectancy growth). Take Chile and Brazil as example. In these countries, the rate went up by 6.9% and 8.1% every year – these are fantastic rates of growth. During the same period, life expectancy increased 25% in Chile and 19% in Brazil compared with Cuba where the increase stood at 17%. In Cuba, the moderate decline in car ownership (-0.1% per annum) would have (very) modestly contributed to the increase of life expectancy. In the other countries, car ownership hindered the increase. (The data is also from the WHO section on Road Safety while the life expectancy data is from the World Bank Database)
This does not alter the trend of life expectancy in Cuba dramatically, but it does alter it in a manner that forces us, once more, to substract from Castro’s accomplishments. This increase would not have been the offspring of the master plan of the dictator, but rather an accidental side-effect springing from policies that depressed living standards so much that Cubans drove less and were less subjected to the risk of dying while driving. However, I am unsure as to whether or not Cubans would regard this as an “improvement”.
Below are the comparisons between Cuba, Chile and Brazil.
The other parts of How Well Has Cuba Managed To Improve Health Outcomes?
Since the passing of Fidel Castro, I have devoted myself to researching a proper assessment of his regime’s achievements in matters of health care. The more I dig, the more I am convinced that his regime has basically been incredibly brilliant at presenting a favorable portrait. The tweaking of the statistics is not blatant or gigantic, it is sufficiently small to avoid alerting demographers (unlike when Davis and Feshbach, Eberstadt and Miller and Velkoff found considerable evidence of data tweaking in the USSR which raised a massive debate). Indeed, a re-computation of life expectancy based on life tables (which I will present in the new few weeks) to adjust for the false reclassification of early neonatal deaths as late fetal deaths (raising the low infant mortality rate by somewhere 28% and 96%) suggests that somewhere between 0.1 and 0.3 years must be knocked off the life expectancy figures. Given that the variations between different measurements available (WHO, World Bank, MINISAP, CIA, FAO) are roughly of that magnitude, it falls within a very reasonable range of errors. This statistical tweaking is combined with an over-dramatization of how terrible the situation was in 1959 (the life expectancy figures vary from 63.9 years to 65.4 years at the beggining of the Castrist regime). But that tweaking is not sufficient to invalidate the massive downward trend. As a result, the majority of public health scholars seem confident in the overall level and trend (and I tend to concur with that statement even if I think things are worse than presented and the slope of the downward trend is too steep).
Those little tweaks have been combined with the use of massive coercive measures on the local population (beautifully described by Katherine Hirschfeld in what should be an example of ethnographic work that economists and policy-makers should rely on because it goes behind the data – see her book Health, Politics, and Revolution in Cuba: 1898-2005) that go from using doctors as tools for political monitoring to the use of abortion against a mother’s will if it may hinder a physician’s chance of reaching the centrally-decided target without forgetting forced isolations for some infectious patients. Such methods are efficient at fighting some types of diseases, but they are associated with institutions that are unable to provide much economic growth which may act as a palliative counter-effects to how choices may make us less healthy (me having the freedom to eat too much salt means I can die earlier, but the type of institutions that let me eat that much salt also avoid infringing on my property rights thus allowing me to improve living standards which is the palliative counter-effect). With such a trade-off, the issue becomes one of the ability of poor countries to improve in the absence of extreme violence as that applied by the Castrist regime.
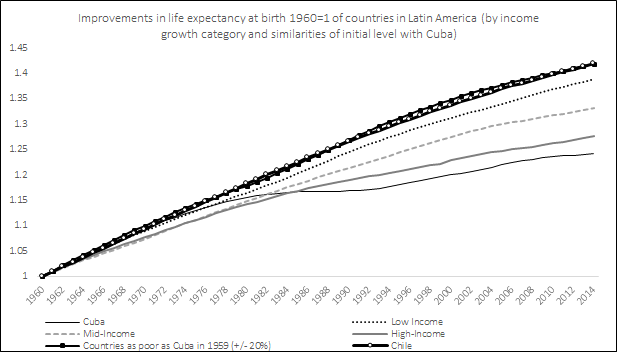
Over the next few weeks, I will publish many re-computations of health statistics to sustain this argument as I write my article. The first one I am doing is the evolution of life expectancy from 1960 to 2014. What I did is that I created comparatives for Cuba based on how much living standards (income per capita). Cuban living less than doubled over that 49 years period (82% increase) from 1959 to 2008 (the latest available data from the high-quality Maddison data). Latin American and Carribean countries that saw their living standards less than double (or even decline) are Argentina (+90%), Bolivia (+87%), El Salvador (+68%), Haïti (-33%), Honduras (+71%), Jamaica (+51%), Nicaragua (-17%) and Venezuela (+7%). This forms the low income group. The remaining countries available are separated in two groups: those whose income increased between 100% and 200% (the mid-income group composed of Brazil, Colombia, Mexico, Peru, Uruguay, Ecuador, Guatemala, Panama and Paraguay) and those whose incomes increased more than 300% (the high-income group composed Chile, Costa Rica, Dominican Republic, Puerto Rico and Trinidad & Tobago). I also compared Cuba with a group of countries that had incomes per capita within 20% of the income per capita of Cuba. So, how did Cuba’s life expectancy increase?
Well, using only the official statistics (which I do not fully trust although they are from the World Bank Development Indicators Database), Cuba life expectancy (which was already pretty high by Latin American standards in 1959) increased 24%. However, all other countries – which were well below Cuba – saw faster increases. The countries that had the least growth in Latin America saw life expectancy increase 38% and the countries that were equally poor as Cuba saw life expectancy increase an impressive 42%. Chile, whose life expectancy was only 57.5 years against Cuba’s 63.9 in 1960, also increased more rapidly (also 42%) and it has now surpassed Cuba (81.5 years against 79.4 years) and what is more impressive is that this rate has increased in a monotonic fashion regardless of changes in political regimes (democracy, socialism, Pinochet, liberal democracy) while Cuba’s rate seems to accelerate and decelerate frequently. Now, this is assuming that the figures for 1960 are correct. I have surveyed the literature and it is hard to find a way to say which of the estimates is the best, but that of the World Bank for 1960 is the lowest. There are other rates, contained in McGuire and Frankel’s work – the highest stands at 65.4 years for 1960. That means that the range of increase of life expectancy in Cuba is between 21.4% and 24.2%. Its not earth-shattering, but it makes Cuba’s achievements less impressive (although it is impressive to keep increase life expectancy from an already-high level). But as you can see, more important improvements could have been generated without recourse to such violent means. In fact, as a post that I will publish this week shows, the decline in car ownership from 1959 to 1988 probably played moderately in favor of the increase in life expectancy while the massive increase in car ownership in all other countries played (all else being equal) in favor of slowing down the increases in life expectancy (but being too poor or making it illegal to import a foreign car is not health care and I deem it improper to consider that this accident from misfortune should be praised).
In a way, what I am saying is that the benefit is not as impressive as claimed. Given the costs that Cubans have to assume for such a policy, anything that makes the benefits look more modest should make more inclined to cast a damning judgment on Castro’s regime.
Coming up (I will add the links as they are published) :
On Black Friday, one of the few remaining tyrants in the world passed away (see the great spread of democracy in the world since 1988). Fidel Castro is a man that I will not mourn nor will I celebrate his passing. What I mourn are the lives he destroyed, the men and women he impoverished, the dreams he crushed and the suffering he inflicted on the innocents. When I state this feeling to others, I am told that he improved life expectancy in Cuba and reduced infant mortality.
To which I reply: why are you proving my point?
The reality that few people understand is that even poor countries can easily reduce mortality with the use of coercive measures available to a centralized dictatorship. There are many diseases (like smallpox) that spread because individuals have a hard time coordinating their actions and cannot prevent free riders (if 90% of people get vaccinated, the 10% remaining gets the protection without having to endure the cost). This type of disease is very easy to fight for a state: force people to get vaccinated.
However, there is a tradeoff to this. The type of institutions that can use violence so cheaply and so efficiently is also the type of institutions that has a hard time creating economic growth and development. Countries with “unfree” institutions are generally poor and grow slowly. Thus, these countries can fight some diseases efficiently (like smallpox and yellow fever), but not other diseases that are related to individual well-being (i.e. poverty diseases). This implies that you get unfree institutions and low rates of epidemics but high levels of poverty and high rates of mortality from tuberculosis, diarrhea, typhoid fever, heart diseases, nephritis.
This argument is basically the argument of Werner Troesken in his great book, The Pox of Liberty. How does it apply to Cuba?
First of all, by 1959, Cuba was already in the top of development indexes for the Americas – a very rich and healthy place by Latin American standards. A large part of the high levels of health indicators were actually the result of coercion. Cuba actually got its very low levels of mortality as a result of the Spanish-American war when the island was occupied by American invaders. They fought yellow fever and other diseases with impressive levels of violence. As Troesken mentions, the rate of mortality fell dramatically in Cuba as a result of this coercion.
Upon taking power in 1959, Castro did exactly the same thing as the Americans. From a public choice perspective, he needed something to shore up support. His policies were not geared towards wealth creation, but they were geared towards the efficient use of violence. As Linda Whiteford and Laurence Branch point out, personal choices are heavily controlled in Cuba in order to achieve these outcomes. Heavy restrictions exist on what Cubans can eat, drink and do. When pregnancies are deemed risky, doctors have to coerce women to undergo abortion in spite of their wishes. Some women are incarcerated in the Casas de Maternidad in spite of their wishes. On top of this, forced sterilization in some cases are an actually documented policy tool. These restrictions do reduce mortality, but they feel like a heavy price for the people. On the other hand, the Castrist regime did get something to brag about and it got international support.
However, when you look at the other side of the tradeoff, you see that death rates from “poverty diseases” don’t seem to have dropped (while they did elsewhere in Latin America). In fact, there are signs that the aggregate infant mortality rates of many other Latin Americans countries collapsed toward the low-levels seen in Cuba when Castro took over in 1959 (here too). Moreover, the crude mortality rate is increasing while infant mortality is decreasing (which is a strong indictment about how much shorter adult lives are in Cuba).
So, yes, Cuba has been very good at reducing mortality from communicable diseases and choice-based outcomes (like how to give birth) that can be reduced by the extreme use of violence. The cost of that use of violence is a low level of development that allows preventable diseases and poverty diseases to remain rampant. Hardly something to celebrate!
Finally, it is also worth pointing two other facts. First of all, economic growth in Cuba has taken place since the 1990s (after decades of stagnation in absolute terms and decline in relative terms). This is the result of the very modest forms of liberalization that were adopted by the Cuban dictatorship as a result of the end of Soviet subsidies. Thus, what little improvements we can see can be largely attributed to those. Secondly, the level of living standards prior to 1990 was largely boosted by the Soviet subsidies but we can doubt how much of it actually went into the hands of the population given that Fidel Castro is worth 900$ million according to Forbes. Thus, yes, Cubans did remain dirt poor during Castro’s reign up to 1990. Thirdly, doctors are penalized for “not meeting quotas” and thus they do lie about the statistics. One thing that is done by the regime is to categorize “infant deaths” as “late fetal deaths” – its basically extending the definition in order to conceal a poorer performance.
Overall, there is nothing to celebrate about Castro’s dictatorship. What some do celebrate is something that was a deliberate political action on the part of Castro to gain support and it came at the cost of personal freedom and higher deaths from preventable diseases and poverty diseases.
