- All-inclusive magic mushroom retreats Max Berlinger, Bloomberg
- What it is to be “young” or “youthful” Eric Schliesser, Digressions & Impressions
- Indian migration and empire Luke de Noronha, Disorder of Things
- Why not rectify past injustices? Bryan Caplan, EconLog
drugs
Nightcap
- Great piece on Latin American history Laurence Blair, BBC History
- The political economy of deep integration (pdf) Maggi & Ossa, NBER
- Democracy in the polycentric city (pdf) Loren King, Journal of Politics
- Here’s what I don’t say Christopher Craig, Threepenny Review
Psychedelics versus modern philosophy
Anyone who studies philosophy has run into the assumption that psychoactive drugs and philosophy go hand-in-hand. Really, after analytic and continental, and whatever other traditions people come up with, there could be another sect, that of “stoner philosophy,” which is something like Mister Rogers, Alan Watts and Bob Ross thrown into a peaceful blender. This is when you’re sitting around getting high, wondering if aliens exist, instead of sitting in a classroom, wondering if other people’s minds exist.
A historical study of this connection, from East to West, would probably scandalize a lot of “serious” philosophers, and show some regular inebriation, but in general, I think the two are opposed (tragically or not). Particularly, the institutionalization of philosophy, when “natural philosophy” and “moral philosophy” etc all became separated some time after Hobbes, is opposed to what it sees as a lay way of thinking about the world. As my philosophy of science professor told me – you become a philosopher when you have your doctorate.
Professional philosophers and “psychonauts” are in opposition to each other. The analytics and continentals have spent centuries building elaborate systems – developing monstrous levels of specificity, so as to make their work completely incomprehensible to the rest of the world – and earning credentials to close the gates of access. Meanwhile, the casual or professional tripper is able to buy a tab for less than $10 and experience, or imagine they experience, market-price existentialism without reading a page of Camus.
The professional philosopher sneers in bad faith at psychedelic profundity because it makes them seem irrelevant.
On the other hand, the inarticulate tripper is not in such a great place. The psychonaut rests on intuition, and is probably not equipt with the critical thinking and logical itinerary to make sense of the journey on the comedown. A trip promises insight but also promises that neither your epistemic priors nor a rational reconstruction will be enough to establish its validity – by its very nature. (Psychedelic knowledge is “revealed,” not “discovered,” right?) You might get an insight that looks good, but is bad, without you knowing it. (I wrote about this in college. Holy shit my writing was bad.)
What happens when you irrationally, psychonautically attach to an idea that’s immune to logical tinkering? If you believe something for irrational reasons you’ll hang on to it for even longer than something that you believed for rational reasons, because new rational reasons can talk you out of a logogenetic idea, but not an irrationally-formed one. Depending on the centrality of the belief, of course.
The psychonaut claims easy knowledge, but could have trouble organizing it in the other, orderly web of belief of his coldly-discovered priors. However, this kind of knowledge has taken a high prestige today, with help from accredited social figures like Steve Jobs dosing LSD. In a way, the win of casual inebriated profundity is a “people’s victory” over the esoteric, pretentious toils of the professional philosophers. If you can figure out Truth by serotonin-fucking yourself on any day of the week then there’s no need to study Heidegger… and there’s even less reason to get a PhD in phenomenology, making institutional philosophy obsolete.
So, philosophers will be opposed to the psychonauts because it trivializes their hard-earned degrees (bad faith), and trivializes all their carefully crafted logic (slightly less bad faith). Psychonauts will be opposed to the philosophers for their specialized field which must explicitly reject such spontaneous routes to knowledge. The people taking psychedelics find themselves fighting some sort of anti-scientific elitism war, doing Feyerabend’s work. The tension is worse with the professional, modern philosophical class, but still exists in general.
A survey of history would show a lot of intertwining, but ultimately, I think the newer age of philosophy has a lot more overlap with other drugs than psychedelics (specifically Epicurean as opposed to elucidatory drugs, e.g. Adderall, analgesics, cocaine) — which is its own interesting question.
Nightcap
- NATO at 70: ten of history’s most important alliances Brandon Christensen, RealClearHistory
- Rethinking American efforts to boost partner militaries Jason Fritz, War on the Rocks
- Brexit is getting worse Tom Harris, CapX
- On the eve of the Great Psychedelic Debate Matthew Blackwell, Quillette
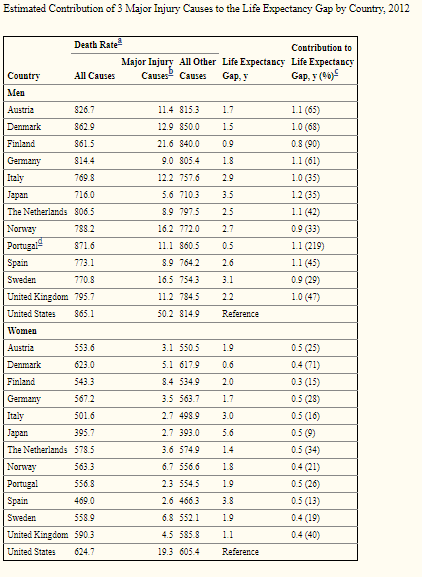
Life expectancy at birth is not a predictor of health care efficiency…
This is going to be a short post to argue that pundits (and some economists) need to stop quoting life expectancy figures to argue for/against a particular health care system. This belief is best exemplified in a recent paper in the Journal of the American Medical Association where Papanicolas et al. (2018) point out that the United States “spent nearly twice as much as 10 high-income countries (…) and performed less well on many population health outcomes”. While the authors make good points about administrative costs, they point out that the US has a low level of life expectancy.
Sure, that is actually true – but Americans tend to die in greater proportions from homicides, drug overdoses and car accidents (Americans drive more than Europeans) than in other rich countries. While these factors of mortality are tragic (except car accidents since Americans seem to prefer the benefits of mobility to the safety of not driving), they are in no way related to the efficiency of health care provision. How much of a deal are these in explaining differences with other industrialized countries? A pretty big deal. For example, these three factors alone account for 64% of the male life expectancy gap between Austria and the United States (see table reproduced below). For women, 26% of the gap between Austria and the United States is explained by these three factors.
The study I cite here only includes three factors. If you add in other factors like drownings among youths (Americans tend to have more drownings than several industrialized countries) which is a result of the fact that Americans are richer and can afford pools (while Europeans tend not to), then you keep explaining away the difference. This is not to say that American health care is great. However, this says that American health care is not as bad as life expectancy outcomes suggest.
Midweek Reader: The Drug War, the Opioid Crisis, and the Moral Hazard of Overdose Treatment
Today, I’m reviving an old series I attempted to start last year that never came to fruition: The midweek reader. A micro-blogging series in which I try to link to stories that are related to each other to provide deeper insight into an issue. This week, we’re looking at the relationship between the Opioid Crisis and the drug war, and the academic debate around a controversial paper finding moral hazard in policies that try to increase access to Naloxone.
- At Harpers Magazine, Brian Gladstone has a fantastic long-form piece looking into how attempts to crack down on opioid addiction by targeting the prescription pain meds have left many patients behind and questioning the mainstream narrative that the rise of opioids was driven primarily by pain prescriptions. A slice:
Yet even the most basic elements of this disaster remain unclear. For while it’s true that the past three decades saw a staggering upsurge in the prescribing of opioid medication, this trend peaked in 2010 and has been declining since: high-dose prescriptions fell by 41 percent between 2010 and 2015. The question, then, is why overdose deaths continue to skyrocket, rising 37 percent over the same period — and whether restricting access to regulated drugs is actually pushing people toward more lethal, unregulated ones, such as fentanyl, heroin, and carfentanil, a synthetic opioid 10,000 times stronger than morphine.
- Similarly, at the Cato Institute, Jeffery A. Singer has a good piece exploring the relationship between America’s War on Drugs and the rise of opioid addictions. He concludes:
Meanwhile, President Trump and most state and local policymakers remain stuck on the misguided notion that the way to stem the overdose rate is to clamp down on the number and dose of opioids that doctors can prescribe to their patients in pain, and to curtail opioid production by the nation’s pharmaceutical manufacturers. And while patients are made to suffer needlessly as doctors, fearing a visit from a DEA agent, are cutting them off from relief, the overdose rate continues to climb.
- At Vox, philosopher Brendan de Kenessey of Harvard has a piece exploring the philosophy of the self and of rational choice to argue that it’s wrong to treat drug addiction as a moral failure. A slice:
We tend to view addiction as a moral failure because we are in the grip of a simple but misleading answer to one of the oldest questions of philosophy: Do people always do what they think is best? In other words, do our actions always reflect our beliefs and values? When someone with addiction chooses to take drugs, does this show us what she truly cares about — or might something more complicated be going on?
- An econometrics working paper by Jennifer L. Doleac of University of Virginia and Anita Mukherjee of the University of Wisconsin released earlier this month, which sparked spirited discussion, investigated the link between opioids and laws increasing access to Naloxone. They found the laws increased measurements of opioid use but did reduce mortality, which they theorize is because Naloxone increases moral hazard for addicts by reducing potential costs of an overdose. However, they conclude:
Our findings do not necessarily imply that we should stop making Naloxone available to individuals suffering from opioid addiction, or those who are at risk of overdose. They do imply that the public health community should acknowledge and prepare for the behavioral effects we find here. Our results show that broad Naloxone access may be limited in its ability to reduce the epidemic’s death toll because not only does it not address the root causes of addiction, but it may exacerbate them. Looking forward, our results suggest that Naloxone’s effects may depend on the availability of local drug treatment: when treatment is available to people who need help overcoming their addiction, broad Naloxone access results in more beneficial effects. Increasing access to drug treatment, then, might be a necessary complement to Naloxone access in curbing the opioid overdose epidemic.
- Alex Gertner, a PhD candidate at UNC-Chaple Hill, published a criticism of Doleac Murkhejee at Vox pointing out that their data linking Naloxone and opioid-related hospital visits are not necessarily due to a casual story involving moral hazard:
The authors find that naloxone access laws lead to more opioid-related emergency department visits, the premise being that naloxone access laws increase opioid overdoses. But there’s a far more likely explanation: People are generally instructed to seek medical care for overdose after receiving naloxone.
Overdose is a general term to describe experiencing the toxic effects of drugs. People can overdose, and often do, without either dying or seeking medical attention. If people who would otherwise overdose without medical attention are instead using naloxone and going to emergency rooms, that’s a good thing.
- The widest-ranging and most thorough critique of Doleac-Murkhejee comes from Frank, Pollack, and Humphries at the Journal of Health Affairs. They argue that the original authors (1) assume too much immediacy in effect of changes in Naloxone laws than is probably warranted (2) ignore a variety of exogenous variables like Medicare expansion. They conclude:
We believe the best interpretation of Doleac and Mukherjee’s findings is that their main treatment variable—naloxone laws—thus far have had little impact on naloxone use or nonmedical opioid use during the period studied. This disappointing pattern commands attention and follow-up from both public health practitioners and public health researchers.
BC’s weekend reads
- the Economist endorses the Liberal Democrats in UK election (in Europe, a liberal democrat is roughly the same thing as a libertarian in the US)
- “One of the most important lessons of Trump’s success is that classically liberal rhetoric and positions were not very important to voters.“
- “It turns out that Westerners are rational, virtuous, and liberty-loving, while Orientals are irrational, vicious, and slavish.“
- The West is indifferent to Afghanistan and Iraq’s world of terror
- Roman slavery, revolution, and magic mushrooms
- What the fuck?
Attention and Motivation
Since reading Pragmatic Thinking and Learning a few years ago, I’ve changed a small but important aspect of my life. I no longer worry about having enough time; I worry about having enough attention. Time devoted to working on a task early in the morning is far more productive than time that would otherwise be spent sleeping devoted to the same task.
In a similar vein, I’ve been coming across tidbits of information related to drugs and attention that have shed some light on this issue for me. For example, what Adderall (basically) does is that it excites your nervous system so that your focus is laser sharp. Suddenly boring tasks like cleaning the house are very easy. Besides ADD drugs, marijuana and LSD are both supposed to do something similar (in the case of LSD, for it to be a useful pharmaceutical would require doses in the sub-Grateful-Dead-concert range… just as you wouldn’t want to eat a handful of Ritalin). [Sorry I don’t have decent citations here… Commenters?]
The point of that last paragraph is to shed some light on the question plaguing those working on improving their own productivity: “How do I increase my motivation?” Anyone who has tried Adderall can tell you that motivation has nothing to do with why they’re cleaning the inside of the oven. They’re just doing it because they can.
What’s my point? Motivation and raw focus are both important, they’re different from one another, but they’re closely tied. Neither is easy to observe from the outside. Recognizing this is obviously important for our own lives. But it is also for how we look at the world as economists.
Six Months A Slave (The Drugs Don’t Work, They Just Make You Worse)
Check out Irfan’s story over at Policy of Truth about six months of addiction to some kind of sleeping pill (I’m a mushrooms and weed man myself, so I know little about pills):
I lay there awhile, let the vertigo wash over me a bit, then popped another 12.5 mg CR Ambien, settling soon enough into another four refreshing hours of non-REM sleep. By 2 am, I was wide awake, reading Jorge Luis Borges (on insomnia), and waiting for the sun to come back up so that I could start yet another vertiginous and sleep deprived day teaching ethics, critical thinking, and aesthetics to students who seemed not to notice that anything was amiss. (Conveniently, I had managed to collapse after class had ended. None of my students saw the collapse happen; I lay on the ground an hour before I was discovered by the instructor who needed to use the classroom after me.)
Read the whole thing. It’s very entertaining.
PS: My title is a reference to a song by The Verve. Don’t ask.

{kind=link}