This is going to be a short post to argue that pundits (and some economists) need to stop quoting life expectancy figures to argue for/against a particular health care system. This belief is best exemplified in a recent paper in the Journal of the American Medical Association where Papanicolas et al. (2018) point out that the United States “spent nearly twice as much as 10 high-income countries (…) and performed less well on many population health outcomes”. While the authors make good points about administrative costs, they point out that the US has a low level of life expectancy.
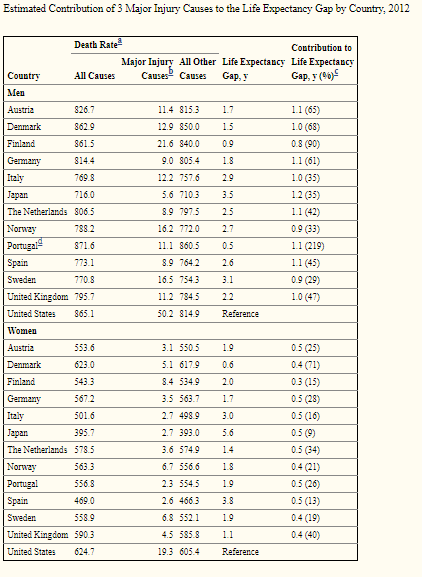
Sure, that is actually true – but Americans tend to die in greater proportions from homicides, drug overdoses and car accidents (Americans drive more than Europeans) than in other rich countries. While these factors of mortality are tragic (except car accidents since Americans seem to prefer the benefits of mobility to the safety of not driving), they are in no way related to the efficiency of health care provision. How much of a deal are these in explaining differences with other industrialized countries? A pretty big deal. For example, these three factors alone account for 64% of the male life expectancy gap between Austria and the United States (see table reproduced below). For women, 26% of the gap between Austria and the United States is explained by these three factors.
The study I cite here only includes three factors. If you add in other factors like drownings among youths (Americans tend to have more drownings than several industrialized countries) which is a result of the fact that Americans are richer and can afford pools (while Europeans tend not to), then you keep explaining away the difference. This is not to say that American health care is great. However, this says that American health care is not as bad as life expectancy outcomes suggest.