Given Zachary’s post on the drug war and opioid crisis, I thought I would share parts of an essay I wrote for a class last semester about Trump’s commission on opioids, which is the first policy step the new administration took in dealing with the issue. It’s edited for links and language and whatnot.
One of the more recent executive steps to combat the opioid crisis — the “abuse” of prescription and illegal opioid-based painkillers — was the creation of The President’s Commission on Combating Drug Addiction and the Opioid Crisis (hereafter, the Commission) two years ago by the Trump administration. The commission, led by Chris Christie, was instituted to investigate the issue further and produce recommendations for the government and pharmaceutical industry. It released its final report in November and seems set to work on opioid use with the same sort of strategies the federal government always treats drugs, except maybe a little more progressive in its consideration of medicinal users. Looking at the Commission’s report, I argue that a refusal to treat unlike cases dissimilarly will lead to less than effective policy.
The President’s Commission
The DEA first asserted that overdose deaths from opioids had reached an epidemic in 2015. In March of last year, Donald Trump signed an executive order establishing the policy of the executive branch to “combat the scourge of drug abuse” and creating The President’s Commission. The Commission is designed to produce recommendations for federal funding, addiction prevention, overdose reversal, recovery, and R&D. Governor Chris Christie of New Jersey served as Chairman alongside Gov. Charlie Baker (R-MA), Gov. Roy Cooper (D-NC), representative Patrick J. Kennedy (D-RI), former deputy director of the Office of National Drug Policy and Harvard professor of psychobiology Bertha Madras, and Florida Attorney General Pam Bondi.
Included in the final report is a short history of opioid use in the United States, characterized by a first crisis in the mid- to late-19th century of “unrestrained … prescriptions,” eventually reversed by medical professionals “combined with federal regulations and law enforcement.” A public distrust of opioids developed afterward, but this was “eroded,” and now the new crisis, traceable to 1999, has become more perilous by innovations since the 19th century: large production firms for prescription drugs, a profitable pharmaceutical industry, cheaper and purer heroin, new fentanyl imports from China.
Since the Commission’s report, several bills have been introduced in the House or Senate currently awaiting judgment (e.g., H.R.4408, H.R.4275, S.2125). Declaring widespread addiction and overdoses to be a national emergency in August, Trump fulfilled one of the interim steps proposed by Christie in an early draft of the report; since, the President has met with drug company executives to discuss nonopiate alternatives for pain relief. Within the next few months we should start to see large scale moves.
Through all of this, the treatment of opioids by the Commission and the US government uses a traditional framing. The National Institute on Drug Abuse (NIDA) defines drug abuse in the following way:
[Use of substances] becomes drug abuse when people use illegal drugs or use legal drugs inappropriately. This includes the repeated use of drugs to produce pleasure, alleviate stress, and/or alter or avoid reality. It also includes using prescription drugs in ways other than prescribed or using someone else’s prescription. Addiction occurs when a person cannot control the impulse to use drugs even when there are negative consequences—the defining characteristic of addiction.
This definition by the federal government does not discriminate between various levels of damaging consumption behavior. The weakness of this definition is that, because all illicit drug consumption is categorized as abuse, there can be no standard for misuse of a black market drug for recreation. An entry-level dose of heroin qualifies as equally “abusive” as a lethal dose because of the binary character of the definition. Other federal agencies give similar definitions; in its report on recommendations for abuse-deterrent generic opioids (see below), the HHS and FDA use a definition of abuse characterized by the “intentional, nontherapeutic use of a drug product or substance, even once, to achieve a desired psychological or physiological effect.” This terminology still characterizes any and all recreational consumption of opioid analgesics as abuse, and not misuse, regardless of dosage or long-term dependency. It will be seen that this is a problem for the success of any sort of policy aimed at quelling usage, and particularly hazardous for the opioid problem.
Legal Background
First, the legal background and a more extensive history. The category “opioid” covers much drug terrain both prescription and illegal. Opioids in the most expansive sense are synthetic derivatives of alkaloids in the opium of the West Asian poppy species Papaver somniferum. Opium resin contains the chemicals morphine, codeine and thebaine. Morphine is the basis for powerful pain relievers like heroin and fentanyl. Codeine is considered less powerful for pain relief but can be used to produce hydrocodone; it also doubles as a cough suppressant. Lastly, thebaine is similar to morphine and is used for oxycodone. 90% of the world’s opium production is in Afghanistan.
All opioids are criminalized under federal Drug Scheduling. Heroin is a Schedule I drug as part of the Controlled Substances Act. Several synthetic opioid drugs that contain hydro- or oxycodone are Schedule II (Vicodin, Dilaudid, OxyContin). Fentanyl is also a Schedule II drug. Heroin is just a brand name for the chemical diacetylmorphine (invented by Bayer), still used as treatment in plenty of developed nations like the United Kingdom and Canada; after heroin was completely criminalized in the United States (“no medical benefits”), synthesized opiate drugs became more popular for prescriptions.
The Pure Food and Drug Act of 1906 introduced labels on medicine containing codeine and opium in general after Chinese immigrant workers introduced the drug to the states. Through 1914, various federal laws restricted opium further until the Harrison Narcotics Tax Act on opium and coca products (which are not narcotics, and the colloquial language has been messed up ever since) effectively criminalized the prescription of opioid products to addicted patients. Shortly afterward, the amount of heroin in the U.S. skyrocketed. Only in recent decades have synthesized opiates occupied the public mind, however. Between 1999 and the present, deaths from overdoses of opioids and opioid-based painkillers like OxyContin, Vicodin, morphine and street heroin have risen almost fourfold.
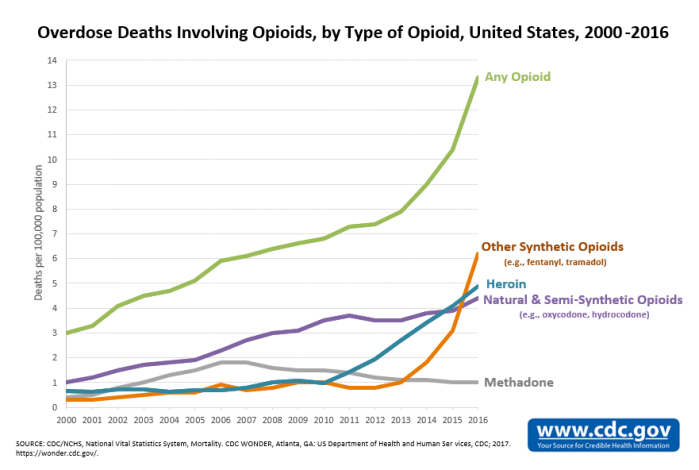
The data on overdoses and deaths does not paint a straightforward picture, and the group “opioid” obscures the different trends between drugs. The CDC classifies data according to four varieties of opioids: natural/semi-synthetic opioid analgesics like morphine, codeine, oxy- or hydrocodone, and oxy- or hydromorphone; synthetic opioid analgesics like tramadol and fentanyl; methadone; and heroin. The last is the only completely illegal opioid. Overdose deaths that have included heroin and completely synthetic opioids have increased exponentially from 2010 and 2013, respectively, while deaths from natural/semi-synthetic opioids and methadone have roughly stabilized or gone down over the last decade. Taken altogether, the deaths from opioid overdoses per 100,000 from 2000 to 2015 have increased from three to eleven people. (As of 2016, natural/semi-synthetic opioid deaths have actually started to go up again, but its still recent in the trend.)
In 2016, the CDC issued guidelines for treating chronic pain that warned physicians against prescribing high dose opioids and suggested talking about health risks. It also advised to “start low and go slow” — a slogan later mocked by John Oliver in a segment on opioids. And, according to a CDC analysis, prescriptions for the most dangerous opioids have dropped 41% from 2010 to 2015, and so have opioid prescriptions in general dropped. This has resulted in patients with physical dependency suffering withdrawal, often without programs to ease the transition to nonopioid pain relievers. Opioid dependants with withdrawal, or average citizens in need of pain relief, often turn to stronger street narcotics, since heroin is the cheaper and stronger alternative to oxycodone. For example, with the drop in first-time OxyContin abuse since 2010, heroin use has spiked. In Maine, a 15% decrease in opioid analgesic overdoses came with a 41% increase in heroin overdoses in 2012. The use of prescribed opioids, then, looks like it might be strongly connected to the use of street narcotics. The Commission, for its credit, notes that “the removal of one substance conceivably will be replaced with another.”
One fact lost in the discussion is that the use of nonmedical opioids has decreased but the amount of overdose deaths has increased. And “opioid epidemic” when discussing overdoses highly obscures that heroin is the major contributor alongside fentanyl — not merely prescription analgesics. We hear a lot about OxyContin and Vicodin, which are actually leveling out (or were until 2015), and less about the drugs which are already policed more, have been policed longer, and cause more physical problems.
What the Commission proposes
In its report, the Commission concludes the goals of its recommendations are “to promote prevention of all drug use with effective education campaigns and restrictions in the supply of illicit and misused drugs.” The President’s Commission doesn’t want to interfere too strongly, despite all of Trump’s suggestions of a revamped drug war. The report notes that coming down hard on opioids will hurt patients with real needs, as has already happened, and, in a way, has happened since 1924. Much of the Commission’s recommendations come from a market approach, e.g. the suggestion (Rec. 19) to reimburse nonopioid pain treatments. The current Centers for Medicare and Medicaid Services (CMS) policy for reimbursement for healthcare providers treats nonopioid, postsurgical pain relief treatments the same as opioid prescriptions, issuing one inclusive payment for all “supplies” at a fixed fee. Nonopioid medications and treatments cost more, and so hospitals opt for dispensing opioids instead. The Commission recommends “adequate reimbursement [for] a broader range of pain management” services, changing the bundle payment policy to accommodate behavioral health treatment, educational programs, “tapering off opioids” and other nonopioid options.
Trump himself suggested an educational approach in a public announcement, which triggered critical comparisons to the failed D.A.R.E. program and “your brain on drugs” commercials. Educational programs are a less coercive option than direct regulation of opioids, but their effectiveness seems to be hit and miss. The Commission cites the Idaho Meth Project from 2007 (ongoing), conducted by a private nonprofit to inform young adults on the health problems associated with methamphetamine use, as a success story: “The Meth Project reports that 94% of teens that are aware of the anti-meth campaign ads say they make them less likely to try or use meth, and that Idaho has experienced a 56% decline in teen meth use since the campaign began.” This meth project is one success story out of many failures. For instance, the Montana Meth Project from 2005, on which the Idaho project was modelled, “accounting for a preexisting downward trend in meth use,” was determined to have “effects on meth use [that] are statistically indistinguishable from zero,” according to an analysis by the National Library of Medicine. Then again, one large scale anti-drug educational campaign, truth, which encourages youth to avoid tobacco, might be having success. Their modern guerrilla tactics are a major improvement on the old model of Partnership for a Drug-Free America.
In another market approach to help recovering addicts reenter society, the Commission recommends decoupling felony convictions and eligibility for certain occupations (Rec. 50). The report cites Section 1128 of the Social Security Act, which prohibits employers that receive funding from federal health programs from hiring past convicts charged with unlawfully manufacturing, distributing or dispensing controlled substances. Any confrontation with law enforcement is a barrier to landing a job — a protected area of discrimination — and government laws that specifically ban their hiring make it worse on ex-users and -dealers trying to get clean. Recommendations like these lessen the role that the state has in keeping ex-convicts out of work.
Much of the funding requested by the President’s Commission is authorized by the Obama administration’s major contribution to combating opioid usage, the Comprehensive Addiction and Recovery Act (CARA), signed into law July 2016 and credited as the “first major federal addiction legislation in 40 years.” CARA helped implement naloxone (an opioid overdose-reversal nail spray) in firefighting departments and strengthen drug monitoring programs.
I’ll post the second half soon, and then a bonus post on my personal favorite solution.


{kind=link}