Here’s the second half of an abridged essay I wrote for a public policy course. First half is here, and next week I’ll write about the FDA’s new enemy, kratom.
Epidemic status
The DEA’s 2015 declaration of an opioid epidemic was the first sign of large-scale federal attention to prescription analgesics, to my knowledge. On the CDC’s official glossary, “outbreak” and “epidemic” are interchangeable: “the occurrence of more cases of disease than expected in a given area or among a specific group of people over a particular period of time.”
The classification of addiction as a disease is sometimes controversial. (See also Adam Alter’s Irresistible for a popularized form of the psychological takes on addiction.) For the opioid problem to be an epidemic, the focus must be the addition rate, and not the overdose or death rate alone. The federal government usually refers to the opioid situation as an epidemic or emergency (which presupposes a value judgment), and when media has covered it (as with the deaths of Philip Seymour Hoffman, Heath Ledger and Prince) they use the same language. One definitive media moment might have been last year, when John Oliver announced for a young progressive crowd that “America is facing an epidemic of addiction to opioids.”
Oliver was referring specifically to addiction — criticizing companies like Purdue Pharma (creator of OxyContin) for misleading or misinformative advertising about addictiveness. But usually it does not seem like the focus is on addiction. As stated, nonmedical usage of opioids is generally down or stabilized from the last couple years, and the problem is mostly overdoses. (True, these are intimately connected.) This might indicate that cutting the pills with other drugs or general inexperienced use are greater problems than general addiction. So, there is an epidemic in the colloquial usage — extensive usage of something which can be harmful — but only questionably in the CDC’s medical definition, as the usage rates are expected to be up as synthesized morphine-, codeine- or thebaine-based pain relievers diversified, and these have mostly stabilized except for heroin (thought as often beyond opioid status) and fully synthetic derivatives which get less attention (fentanyl, tramadol).
Why the standard of abuse fails
John Oliver — worthy to talk about because much of the public plausibly started paying attention after his episode — noted that the pills are assigned to patients and then, even if the patient doesn’t develop an addiction, they end up in the “wrong hands.” What happens at this point? The Commission recommends that companies design their prescription drugs for “abuse-deterrent” formulations (ADF). After spikes in opioid abuse, Purdue Pharma and other companies began researching mechanisms to prevent abusers from easily obtaining a recreational high by tampering with the pill or capsule. In a public statement, FDA commissioner Scott Gottlieb asserted that the administration’s focus is on “decreasing unnecessary exposure to opioids,” but, recognizing the real role that prescription opioids play in pain relief, Gottlieb continues that “until we’re able to find new nonopioid forms of pain management … it’s critical that that we also continue to promote the development of opioids that are harder to manipulate and abuse, and take steps to encourage their use over opioids that don’t offer any form of deterrence.” Some of these abuse-deterrent options are crush resistance or wax coating to make dissolving more difficult.
However, opioid abuse comes in two forms which are conflated by the legal language. The first is when a patient takes more than their recommended allocation or takes it in the wrong way. The second is when someone with or without a prescription consumes them purely for recreation. Many drug savvy abusers of the second variety have adapted methods to get a recreational high but avoid potential health risks, the most popular method being “cold water extraction” (CWE). Most opioid pills contain both a synthesized opium alkaloid (from morphine, codeine or thebaine) and acetaminophen: Percocet contains oxycodone and paracetamol; Vicodin contains hydrocodone and paracetamol. The acetaminophen or APAP has no recreational benefits (a pure pain reliever/fever reducer) and can cause severe liver problems in large quantities, so recreational users will extract the opium alkaloid by crushing the pill, dissolving it in distilled water, chilling it to just above freezing, and filtering out the uncrystallized APAP from the synthesized opium. This way a greater quantity of the opioid can be ingested without needlessly consuming acetaminophen. Other recreational users that want less of the opium derivative can proceed without CWE and insufflate or orally ingest the particular pills.
ADFs might be able to dent the amount of abusers of the second variety. If the pills are harder to crush (the route of Purdue’s 2010 OxyContin release) or, for capsules, the interior balls are harder to dissolve (the route of Collegium Pharmaceutical’s Xtampza), amateur or moderately determined oxycodone enthusiasts may find the buzz is not worth the labor. As the Commission observes, more than 50% of prescription analgesic misusers get them from friends and family (p. 41) — these are not hardcore aficionados, but opportunists who might be dissuaded by simple anti-abuse mechanisms. Abusers of the first variety, though, are unaffected: at least in the short term, their abuse rests on slightly-over-the-recommended doses or a natural tendency to develop an addiction or non-medical physical dependency. And, if the political core of the opioid emergency is patients that develop an addiction accidentally (those that stay addicted to pharmaceuticals and those that graduate to heroin), abuse-deterrent focuses are unlikely to create real change in addiction rates. It could even have the unintended consequence of higher overdose deaths for amateur narcotics recreationalists, who aren’t skilled enough to perform extractions and opt to consume more pills in one sitting instead.
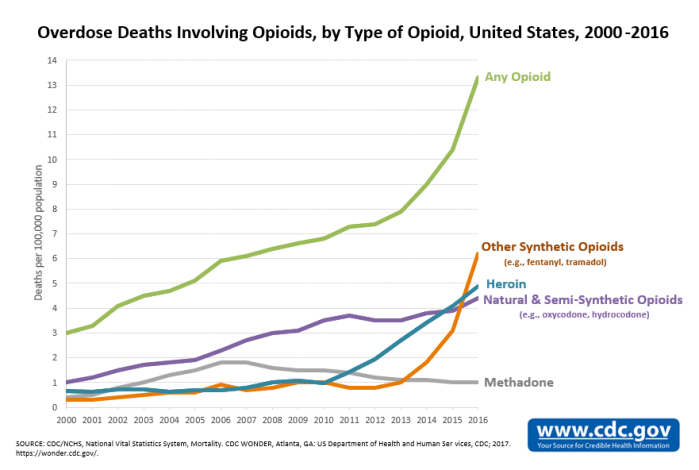
And furthermore, ADFs can be incorporated into the naturals and synthetics that are usually bonded with APAP like codeine, oxycodone, hydrocodone and tramadol, but cannot for the drugs that come in pure form like heroin or fentanyl. And those are the problem drugs. The NIDA research on drugs involved in overdose deaths across the board, for one, shows that overdose deaths are on the rise as a whole (except for methadone), and also that the synthetic opioids are much more deadly than the naturals and semi-synthetics: fentanyl is the biggest prescription analgesic killer (it’s much more potent than morphine, and tramadol is not very good for recreation).
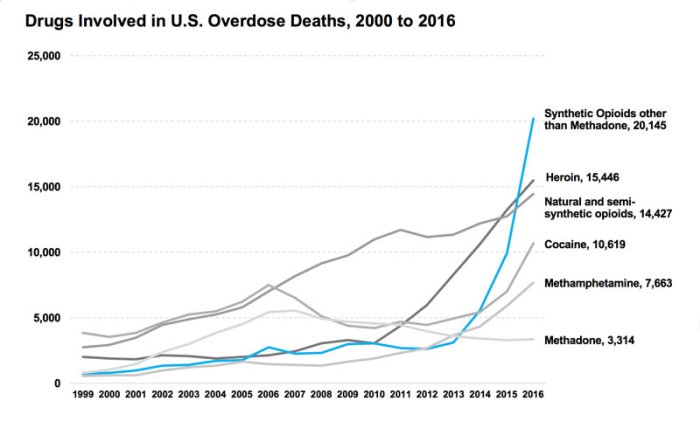
(This graph also shows, however, that the natural/semi-synthetic usage rate was possibly leveling out but resuscitated in 2015.) So ADFs are useless for the drugs most massively causing the “opioid epidemic.” Making them harder to abuse only dents the second category of abuser, and does not limit their addictiveness for those prescribed them for postsurgical pain or otherwise.
Moreover, from a libertarian standpoint, the second category of abuser does not really belong in the “public health crisis” discussion. Those who knowingly consume opioids for recreation are not a problem, they are participants in a pleasure-seeking activity that doesn’t tread on others. So long as their costs are not imposed on other people, it might be better to separate them from the “epidemic” status. Blurring the lines between the groups that fall under “abusive” means that those with a side-interest in OxyContin on Friday nights are lumped in with addicts suffering from physical dependency. Someone who has a glass of wine each night is not “abusing” alcohol, but we can recognize someone who is an alcoholic; the same distinction should be applied medically to opioid users. By painting all consumers outside of direct medical usage as “abusers,” there can be no standard for misuse, and thus no way for a recreationalist to know how much is too much, when health problems might set in, if they are really trapped in their recreation, etc. Research and knowledge are threatened by the legal treatment and classification.
Conclusion
To summarize, the government terminology of “abuse” obscures a legitimate distinction that is justified on both medical-political and civil liberty grounds. Some of the approaches in the Commission report, like the market-based CMS package recommendation, will likely succeed at quelling opioid exposure (and thus addiction and overdoses), while other maneuvers like an education campaign or ADFs should be treated with cautious skepticism. The trends show that heroin and fentanyl are actually the biggest contributors to the opioid epidemic, although semi-synthetics are climbing again in overdose deaths after leaning toward stabilization two years ago. Evidence that prescription abuse and street use are linked, as well as testimony from former addicts, indicates that drug users easily swing between the legal and black market.