- This is your US Constitution on drugs Ilya Shapiro, National Affairs
- The early years of Communist Party rule Ian Johnson, NY Times
- Why Leftists prefer and even encourage “cancel culture” Chris Bertram, Crooked Timber
- The rumour about the Jews Francesca Trivellato, Aeon
- New light on the dark interwar years Tony Barber, Financial Times
War on Drugs
Nightcap
- Jack Schwartz on the weaknesses of the Mathematical Mind David Glasner, Uneasy Money
- Did the Thirty Glorious Years actually exist? Vincent Geloso, NOL
- A hidden cost of the War on Drugs Vincent Geloso, NOL
- Star Trek did more for the cultural advancement of women than government policies Vincent Geloso, NOL
Blame it on Rio
I grew up in Rio de Janeiro in a very middle-class neighborhood. Not the fanciest one, but also not the poorest. Very much in the middle. This neighborhood also had the characteristic of being surrounded by hills. Many if not most hills in Rio de Janeiro have favelas. Favelas are poor neighborhoods that are formed by poor people who mostly want to live close to where the jobs are. Because I grew up in a middle-class neighborhood, studied in middle-class schools and had a middle-class family I was in danger of only knowing middle-class people. The thing that prevented me from that the most was going to church. In church, I lived with people from all kind of social backgrounds – including people who lived in favelas.
The history of Rio de Janeiro is mostly a history of expansion from the area we today call downtown. On several occasions, poor people (including my grandfather and his mother) were relocated (or frankly expelled) from their houses by the government that wanted to make some urban reform. People faced two options: to be relocated to far removed areas, far away from their jobs, or to occupy some undeveloped area in the vicinities of where they previously lived and form a favela.
Because Rio de Janeiro is the historic capital of Brazil, it received a lot of investment by governments over the decades. Many governments wanted to make it a vitrine of Brazil’s development. Also, Brazil has a strong history of developmentalism. Especially since Getúlio Vargas, who rule the country from 1930 to 1945 and again from 1951 to 1954, Brazilian presidents tend to believe that it is their job to bring economic development to the country. The higher the GDP growth, the best. I mean, who am I to say that GDP growth is a bad thing?! But we have a lot of stories worldwide of countries that grew too fast in too little time leading among other things to major population dislocations and new pockets of poverty around great cities. Lagos, in Nigeria, is a textbook example. So is Caracas, in Venezuela. So is Rio de Janeiro. This kind of development is pretty much like using steroids: the results are fast, but the side effects are terrible. Fernando Henrique Cardoso tried to “flip the page” from Vargas in the 1990s, but Lula da Silva and Dilma Rousseff returned to developmentalist policies in the 2000s. Even Jair Bolsonaro often talks as a developmentalist, apparently a tic from his military years. Anyways, developmentalism led to the fast growth of Rio de Janeiro over the decades – and the formation of new favelas.
One of the best stories of developmentalism in Rio de Janeiro is the neighborhood of Barra da Tijuca. Until the 1960s this part of the city, caught between the hills and the ocean, was basically desert. That’s when the government commissioned the architect and urbanist Lucio Costa to develop the area. Mr. Costa was also responsible for designing the city of Brasília, and it shows: Brasília and Barra da Tijuca are fairly similar. Not my kind of city or neighborhood. It’s very hard or even impossible to explore Barra da Tijuca on foot. Its area is roughly the size of Manhattan, but it has no subway lines. The bus lines are not very dependable. The city blocks are very large. Everything is very distant.
In my evaluation, Mr. Costa thought that he was God. Brasília and Barra and very interesting if looked from above, from the sky. But if you are on the ground level and don’t have a car, they are just not friendly. But that’s how modernists (including socialists) are: they swear they love humanity but hate human beings.
The news that the government was developing the Barra da Tijuca area spread fast. Many families came to the region looking for jobs in construction. Many of them settled in the vicinity of Rio das Pedras. Rio das Pedras became one of the main favelas of the region. In the absence of government, people started to organize themselves in neighborhood associations. Even with most of the construction projects done, the families never left. Barra da Tijuca became an affluent neighborhood with many jobs. Alongside came drug trafficking.
The “pre-history” of drug trafficking in Rio de Janeiro is almost idyllic. You just have to watch the movie City of God (2002). Of course, one could not sell drugs in fancy neighborhoods like Ipanema or Copacabana, where the government is strongly present.
So, most drug trafficking happened in the favelas, including Rio das Pedras. The first generation of drug dealers was mostly respectful towards residents of the favelas and other poor neighborhoods. Some even became legendary for pacifying the neighborhoods from other forms of crime: because they didn’t want to have trouble with the police, drug dealers would punish criminals themselves. However, this changed very fast. The dispute for territory led drug dealers to become more and more violent.
In response to drug dealers and the slackness of the government, people organized in militias. What once were neighborhood associations became paramilitary organizations. Just like happened with the drug dealers, the vigilantes were initially friendly towards the people living in the neighborhoods. However, this changed very fast. The dispute for territory led militias to become more and more violent. Eventually, drug dealers and militias became mostly indistinguishable. Some militia leaders entered politics.
Marcelo Freixo, a Rio de Janeiro politician of the PSOL (Socialism and Liberty Party – as I said before, a contradiction in terms) rose to fame in the 2000s for presiding over a parliamentary inquiry on the militias. Mr. Freixo had a character inspired on him in the movie Elite Squad 2 (2010). The first Elite Squad (2007) was a very good movie. The sequel, not so much. Elite Squad is somewhat based on real events and tells the story of (what else?) BOPE, an elite squad in the Rio de Janeiro military police (somewhat analogous to the SWAT), especially during the visit of Pope John Paul II to the city in the late 1990s. The movie has some similarities to Black Hawk Down (2001). If you haven’t watched it and want to be spoil free, you might want to skip to the next paragraph.
Pope John Paul II decided to stay in a dangerous neighborhood, surrounded by favelas. The BOPE was responsible for his security. Although disagreeing with the strategic intelligence of allowing the Pope to stay in a dangerous region of the city, the squad did its job. In very military fashion, “orders are orders”. The movie shows the police officers as very dubious figures: they are extremely violent and often disrespectful towards citizens. But they are also very honest and dutybound. Captain Nascimento, the main character, is a tragic figure. He became a police officer to protect innocent citizens. He discovers that by obeying orders he is often just putting his life in risk for very little or no results. Worse, he is misunderstood by all those around him, including his family.
Even his son ends up calling him a fascist. Elite Squad also portrays the drug dealers in a nuanced way. They are violent and vengeful, but Captain Nascimento himself understands that no one grows up dreaming about becoming a drug dealer. Drug dealers and BOPE members fight a private war and ironically might be the only ones to truly understand one another. The real villains of the movie are the upper-middle class youngsters who use drugs, financing the drug dealers who the BOPE fights. It is against them that the police officers direct most of their rage.
So, I believe that Elite Squad is a very good movie, that pictures quite well how life in Rio de Janeiro is for many people. Most of the time it is hard to precisely identify villains or heroes. However, no wonder, despite being very popular, the movie was trashed by leftist intellectuals who called it fascist. The sequel gains in quality in almost everything but the characters, and this makes it worse than the original. The villains are completely villainous and the heroes, heroic. It lacks the nuances of the original. The character inspired by Marcelo Freixo is morally perfect. The vigilantes whom he fights are cartoonish evil.
Brazilian and international media gave much attention last year to the assassination of Marielle Franco, a Rio de Janeiro politician who, just like Mr. Freixo, was a member of the PSOL. Ms. Franco’s assassination, like any other, is a tragedy. The police investigation is still ongoing, and no one really knows who killed her, but it seems very likely that she was murdered by members of a militia. Despite what international media might lead one to believe, Ms. Franco was far from being the first Rio de Janeiro politician to be murdered in the last few years. Mr. Freixo himself is under police protection for many years now. Other politicians from several political parties were not so lucky and didn’t receive the same attention from the media. The left’s last blow against president Jair Bolsonaro is to say that one of his sons, Flávio Bolsonaro, is somehow connected to Ms. Franco assassination. In their narrative, Flávio would be connected to militias who in turn killed Ms. Franco. All things are possible. Not all are plausible. Definitely, not all are proven. To be honest, there are people in the right saying that Jean Wyllys, also from the PSOL, is connected to Jair Bolsonaro’s assassination attempt last September. Maybe they should all go have a drink together. They have much in common.
Making a generalization (but I hope not an overgeneralization), politicians and intellectuals from the left tend to romanticize drug dealers. They are pictured as social victims or social bandits, almost Robin Hoods. On the other hand, they vilify the militias in a cartoonish way. Just like Elite Squad 2. I began this text mentioning that going to church prevented me from entirely growing in a middle-class bubble. Because of that, I heard people saying that old drug dealers had at least some sense of justice. Younger ones (sometimes as young as 16 years old) are almost animals, psychopaths without any sense of empathy. If you watched The Godfather trilogy you know what I mean. I also heard people frustrated with the government, that offered no protection against criminals. The same people were (at least initially) supportive of militias.
Politicians in the right, in turn, consider unimaginable to legalize any drug. But on the other hand, they were very slow to understand the danger of the militias, and citizens making justice with their own hands in general.
So, this is a story about Rio de Janeiro, one of Brazil’s most important cities. For decades politicians believed it was their job to bring economic development to the country – and to the city. This led to fast economic growth, which in turn led to the development of favelas. Favelas are areas where the official government is generally not present.
Therefore, its residents form neighborhood associations. Favelas are also places where, because of the lack of government, drug dealers can work in relative peace. However, over time drug dealers become more and more violent in their dispute for territory. The neighborhood associations, in turn, become militias. And the militias quite often become mafias. Some politicians rise to fame fighting these mafias, but the policies they defend are the same that begin this story in the first place. Politicians on the right are accused of dangerous liaisons. And no one seems to be willing to limit government to its primary function of protecting life and private property.
Nightcap
- The world’s first political risk consultants John Hulsman, Aeon
- Why We Should Say Yes to Drugs Andrew Sullivan, Daily Intelligencer
- A primer on fentanyl(s) Mark Kleiman, Reality-Based Community
- Moral responsibility Scott Sumner, EconLog
Pot smoking and freedom: ‘Murica!
My latest Tuesday column over at RealClearHistory takes aim at the history of marijuana in the United States. I’ve got a 600 word limit, but hopefully I packed in plenty of info. Here’s an excerpt:
During the much-loathed Prohibition era (1920-33), marijuana was targeted along with alcohol and other substances deemed immoral by bootleggers and Baptists. Unlike alcohol, which was re-legalized in 1933, marijuana ended up in a legal limbo that continues to this day. The legal, political, economic, and cultural battles surrounding marijuana use in the United States have helped shape three generations of lawyers, businesspeople, activists, academics, and medical professionals. Thanks to the questions posed by marijuana prohibition, rigorous and creative arguments in favor of the drug’s legalization have contributed to a better understanding of our federal system of government, of Judeo-Christian morality, and non-Western ethical systems (pot-smoking “Buddhists” are practically cliche today), of the human body and especially the brain, of global trading networks throughout history, and of intercultural exchange and communication. Freedom still defines us as a society. Freedom binds Americans together. Freedom drives our conversations and our institutional actors. This may be difficult to remember as the news cycle grows ever more sensational, but this quiet, humble truth still remains.
Please, read the rest.
The President’s commission on opioids (2/2)
Here’s the second half of an abridged essay I wrote for a public policy course. First half is here, and next week I’ll write about the FDA’s new enemy, kratom.
Epidemic status
The DEA’s 2015 declaration of an opioid epidemic was the first sign of large-scale federal attention to prescription analgesics, to my knowledge. On the CDC’s official glossary, “outbreak” and “epidemic” are interchangeable: “the occurrence of more cases of disease than expected in a given area or among a specific group of people over a particular period of time.”
The classification of addiction as a disease is sometimes controversial. (See also Adam Alter’s Irresistible for a popularized form of the psychological takes on addiction.) For the opioid problem to be an epidemic, the focus must be the addition rate, and not the overdose or death rate alone. The federal government usually refers to the opioid situation as an epidemic or emergency (which presupposes a value judgment), and when media has covered it (as with the deaths of Philip Seymour Hoffman, Heath Ledger and Prince) they use the same language. One definitive media moment might have been last year, when John Oliver announced for a young progressive crowd that “America is facing an epidemic of addiction to opioids.”
Oliver was referring specifically to addiction — criticizing companies like Purdue Pharma (creator of OxyContin) for misleading or misinformative advertising about addictiveness. But usually it does not seem like the focus is on addiction. As stated, nonmedical usage of opioids is generally down or stabilized from the last couple years, and the problem is mostly overdoses. (True, these are intimately connected.) This might indicate that cutting the pills with other drugs or general inexperienced use are greater problems than general addiction. So, there is an epidemic in the colloquial usage — extensive usage of something which can be harmful — but only questionably in the CDC’s medical definition, as the usage rates are expected to be up as synthesized morphine-, codeine- or thebaine-based pain relievers diversified, and these have mostly stabilized except for heroin (thought as often beyond opioid status) and fully synthetic derivatives which get less attention (fentanyl, tramadol).
Why the standard of abuse fails
John Oliver — worthy to talk about because much of the public plausibly started paying attention after his episode — noted that the pills are assigned to patients and then, even if the patient doesn’t develop an addiction, they end up in the “wrong hands.” What happens at this point? The Commission recommends that companies design their prescription drugs for “abuse-deterrent” formulations (ADF). After spikes in opioid abuse, Purdue Pharma and other companies began researching mechanisms to prevent abusers from easily obtaining a recreational high by tampering with the pill or capsule. In a public statement, FDA commissioner Scott Gottlieb asserted that the administration’s focus is on “decreasing unnecessary exposure to opioids,” but, recognizing the real role that prescription opioids play in pain relief, Gottlieb continues that “until we’re able to find new nonopioid forms of pain management … it’s critical that that we also continue to promote the development of opioids that are harder to manipulate and abuse, and take steps to encourage their use over opioids that don’t offer any form of deterrence.” Some of these abuse-deterrent options are crush resistance or wax coating to make dissolving more difficult.
However, opioid abuse comes in two forms which are conflated by the legal language. The first is when a patient takes more than their recommended allocation or takes it in the wrong way. The second is when someone with or without a prescription consumes them purely for recreation. Many drug savvy abusers of the second variety have adapted methods to get a recreational high but avoid potential health risks, the most popular method being “cold water extraction” (CWE). Most opioid pills contain both a synthesized opium alkaloid (from morphine, codeine or thebaine) and acetaminophen: Percocet contains oxycodone and paracetamol; Vicodin contains hydrocodone and paracetamol. The acetaminophen or APAP has no recreational benefits (a pure pain reliever/fever reducer) and can cause severe liver problems in large quantities, so recreational users will extract the opium alkaloid by crushing the pill, dissolving it in distilled water, chilling it to just above freezing, and filtering out the uncrystallized APAP from the synthesized opium. This way a greater quantity of the opioid can be ingested without needlessly consuming acetaminophen. Other recreational users that want less of the opium derivative can proceed without CWE and insufflate or orally ingest the particular pills.
ADFs might be able to dent the amount of abusers of the second variety. If the pills are harder to crush (the route of Purdue’s 2010 OxyContin release) or, for capsules, the interior balls are harder to dissolve (the route of Collegium Pharmaceutical’s Xtampza), amateur or moderately determined oxycodone enthusiasts may find the buzz is not worth the labor. As the Commission observes, more than 50% of prescription analgesic misusers get them from friends and family (p. 41) — these are not hardcore aficionados, but opportunists who might be dissuaded by simple anti-abuse mechanisms. Abusers of the first variety, though, are unaffected: at least in the short term, their abuse rests on slightly-over-the-recommended doses or a natural tendency to develop an addiction or non-medical physical dependency. And, if the political core of the opioid emergency is patients that develop an addiction accidentally (those that stay addicted to pharmaceuticals and those that graduate to heroin), abuse-deterrent focuses are unlikely to create real change in addiction rates. It could even have the unintended consequence of higher overdose deaths for amateur narcotics recreationalists, who aren’t skilled enough to perform extractions and opt to consume more pills in one sitting instead.
And furthermore, ADFs can be incorporated into the naturals and synthetics that are usually bonded with APAP like codeine, oxycodone, hydrocodone and tramadol, but cannot for the drugs that come in pure form like heroin or fentanyl. And those are the problem drugs. The NIDA research on drugs involved in overdose deaths across the board, for one, shows that overdose deaths are on the rise as a whole (except for methadone), and also that the synthetic opioids are much more deadly than the naturals and semi-synthetics: fentanyl is the biggest prescription analgesic killer (it’s much more potent than morphine, and tramadol is not very good for recreation).
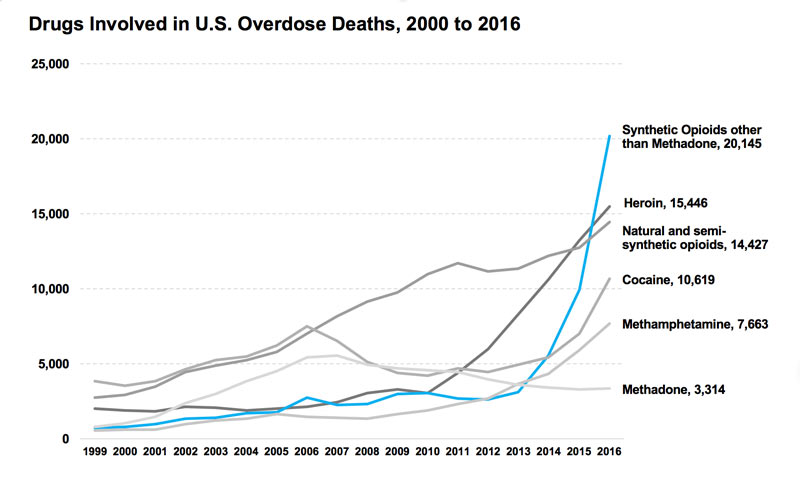
(This graph also shows, however, that the natural/semi-synthetic usage rate was possibly leveling out but resuscitated in 2015.) So ADFs are useless for the drugs most massively causing the “opioid epidemic.” Making them harder to abuse only dents the second category of abuser, and does not limit their addictiveness for those prescribed them for postsurgical pain or otherwise.
Moreover, from a libertarian standpoint, the second category of abuser does not really belong in the “public health crisis” discussion. Those who knowingly consume opioids for recreation are not a problem, they are participants in a pleasure-seeking activity that doesn’t tread on others. So long as their costs are not imposed on other people, it might be better to separate them from the “epidemic” status. Blurring the lines between the groups that fall under “abusive” means that those with a side-interest in OxyContin on Friday nights are lumped in with addicts suffering from physical dependency. Someone who has a glass of wine each night is not “abusing” alcohol, but we can recognize someone who is an alcoholic; the same distinction should be applied medically to opioid users. By painting all consumers outside of direct medical usage as “abusers,” there can be no standard for misuse, and thus no way for a recreationalist to know how much is too much, when health problems might set in, if they are really trapped in their recreation, etc. Research and knowledge are threatened by the legal treatment and classification.
Conclusion
To summarize, the government terminology of “abuse” obscures a legitimate distinction that is justified on both medical-political and civil liberty grounds. Some of the approaches in the Commission report, like the market-based CMS package recommendation, will likely succeed at quelling opioid exposure (and thus addiction and overdoses), while other maneuvers like an education campaign or ADFs should be treated with cautious skepticism. The trends show that heroin and fentanyl are actually the biggest contributors to the opioid epidemic, although semi-synthetics are climbing again in overdose deaths after leaning toward stabilization two years ago. Evidence that prescription abuse and street use are linked, as well as testimony from former addicts, indicates that drug users easily swing between the legal and black market.
The President’s commission on opioids (1/2)
Given Zachary’s post on the drug war and opioid crisis, I thought I would share parts of an essay I wrote for a class last semester about Trump’s commission on opioids, which is the first policy step the new administration took in dealing with the issue. It’s edited for links and language and whatnot.
One of the more recent executive steps to combat the opioid crisis — the “abuse” of prescription and illegal opioid-based painkillers — was the creation of The President’s Commission on Combating Drug Addiction and the Opioid Crisis (hereafter, the Commission) two years ago by the Trump administration. The commission, led by Chris Christie, was instituted to investigate the issue further and produce recommendations for the government and pharmaceutical industry. It released its final report in November and seems set to work on opioid use with the same sort of strategies the federal government always treats drugs, except maybe a little more progressive in its consideration of medicinal users. Looking at the Commission’s report, I argue that a refusal to treat unlike cases dissimilarly will lead to less than effective policy.
The President’s Commission
The DEA first asserted that overdose deaths from opioids had reached an epidemic in 2015. In March of last year, Donald Trump signed an executive order establishing the policy of the executive branch to “combat the scourge of drug abuse” and creating The President’s Commission. The Commission is designed to produce recommendations for federal funding, addiction prevention, overdose reversal, recovery, and R&D. Governor Chris Christie of New Jersey served as Chairman alongside Gov. Charlie Baker (R-MA), Gov. Roy Cooper (D-NC), representative Patrick J. Kennedy (D-RI), former deputy director of the Office of National Drug Policy and Harvard professor of psychobiology Bertha Madras, and Florida Attorney General Pam Bondi.
Included in the final report is a short history of opioid use in the United States, characterized by a first crisis in the mid- to late-19th century of “unrestrained … prescriptions,” eventually reversed by medical professionals “combined with federal regulations and law enforcement.” A public distrust of opioids developed afterward, but this was “eroded,” and now the new crisis, traceable to 1999, has become more perilous by innovations since the 19th century: large production firms for prescription drugs, a profitable pharmaceutical industry, cheaper and purer heroin, new fentanyl imports from China.
Since the Commission’s report, several bills have been introduced in the House or Senate currently awaiting judgment (e.g., H.R.4408, H.R.4275, S.2125). Declaring widespread addiction and overdoses to be a national emergency in August, Trump fulfilled one of the interim steps proposed by Christie in an early draft of the report; since, the President has met with drug company executives to discuss nonopiate alternatives for pain relief. Within the next few months we should start to see large scale moves.
Through all of this, the treatment of opioids by the Commission and the US government uses a traditional framing. The National Institute on Drug Abuse (NIDA) defines drug abuse in the following way:
[Use of substances] becomes drug abuse when people use illegal drugs or use legal drugs inappropriately. This includes the repeated use of drugs to produce pleasure, alleviate stress, and/or alter or avoid reality. It also includes using prescription drugs in ways other than prescribed or using someone else’s prescription. Addiction occurs when a person cannot control the impulse to use drugs even when there are negative consequences—the defining characteristic of addiction.
This definition by the federal government does not discriminate between various levels of damaging consumption behavior. The weakness of this definition is that, because all illicit drug consumption is categorized as abuse, there can be no standard for misuse of a black market drug for recreation. An entry-level dose of heroin qualifies as equally “abusive” as a lethal dose because of the binary character of the definition. Other federal agencies give similar definitions; in its report on recommendations for abuse-deterrent generic opioids (see below), the HHS and FDA use a definition of abuse characterized by the “intentional, nontherapeutic use of a drug product or substance, even once, to achieve a desired psychological or physiological effect.” This terminology still characterizes any and all recreational consumption of opioid analgesics as abuse, and not misuse, regardless of dosage or long-term dependency. It will be seen that this is a problem for the success of any sort of policy aimed at quelling usage, and particularly hazardous for the opioid problem.
Legal Background
First, the legal background and a more extensive history. The category “opioid” covers much drug terrain both prescription and illegal. Opioids in the most expansive sense are synthetic derivatives of alkaloids in the opium of the West Asian poppy species Papaver somniferum. Opium resin contains the chemicals morphine, codeine and thebaine. Morphine is the basis for powerful pain relievers like heroin and fentanyl. Codeine is considered less powerful for pain relief but can be used to produce hydrocodone; it also doubles as a cough suppressant. Lastly, thebaine is similar to morphine and is used for oxycodone. 90% of the world’s opium production is in Afghanistan.
All opioids are criminalized under federal Drug Scheduling. Heroin is a Schedule I drug as part of the Controlled Substances Act. Several synthetic opioid drugs that contain hydro- or oxycodone are Schedule II (Vicodin, Dilaudid, OxyContin). Fentanyl is also a Schedule II drug. Heroin is just a brand name for the chemical diacetylmorphine (invented by Bayer), still used as treatment in plenty of developed nations like the United Kingdom and Canada; after heroin was completely criminalized in the United States (“no medical benefits”), synthesized opiate drugs became more popular for prescriptions.
The Pure Food and Drug Act of 1906 introduced labels on medicine containing codeine and opium in general after Chinese immigrant workers introduced the drug to the states. Through 1914, various federal laws restricted opium further until the Harrison Narcotics Tax Act on opium and coca products (which are not narcotics, and the colloquial language has been messed up ever since) effectively criminalized the prescription of opioid products to addicted patients. Shortly afterward, the amount of heroin in the U.S. skyrocketed. Only in recent decades have synthesized opiates occupied the public mind, however. Between 1999 and the present, deaths from overdoses of opioids and opioid-based painkillers like OxyContin, Vicodin, morphine and street heroin have risen almost fourfold.
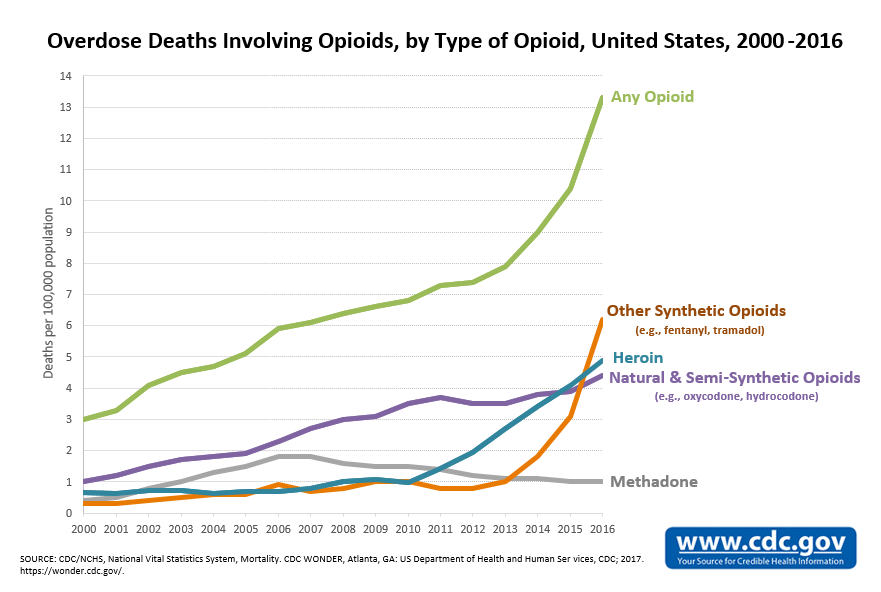
The data on overdoses and deaths does not paint a straightforward picture, and the group “opioid” obscures the different trends between drugs. The CDC classifies data according to four varieties of opioids: natural/semi-synthetic opioid analgesics like morphine, codeine, oxy- or hydrocodone, and oxy- or hydromorphone; synthetic opioid analgesics like tramadol and fentanyl; methadone; and heroin. The last is the only completely illegal opioid. Overdose deaths that have included heroin and completely synthetic opioids have increased exponentially from 2010 and 2013, respectively, while deaths from natural/semi-synthetic opioids and methadone have roughly stabilized or gone down over the last decade. Taken altogether, the deaths from opioid overdoses per 100,000 from 2000 to 2015 have increased from three to eleven people. (As of 2016, natural/semi-synthetic opioid deaths have actually started to go up again, but its still recent in the trend.)
In 2016, the CDC issued guidelines for treating chronic pain that warned physicians against prescribing high dose opioids and suggested talking about health risks. It also advised to “start low and go slow” — a slogan later mocked by John Oliver in a segment on opioids. And, according to a CDC analysis, prescriptions for the most dangerous opioids have dropped 41% from 2010 to 2015, and so have opioid prescriptions in general dropped. This has resulted in patients with physical dependency suffering withdrawal, often without programs to ease the transition to nonopioid pain relievers. Opioid dependants with withdrawal, or average citizens in need of pain relief, often turn to stronger street narcotics, since heroin is the cheaper and stronger alternative to oxycodone. For example, with the drop in first-time OxyContin abuse since 2010, heroin use has spiked. In Maine, a 15% decrease in opioid analgesic overdoses came with a 41% increase in heroin overdoses in 2012. The use of prescribed opioids, then, looks like it might be strongly connected to the use of street narcotics. The Commission, for its credit, notes that “the removal of one substance conceivably will be replaced with another.”
One fact lost in the discussion is that the use of nonmedical opioids has decreased but the amount of overdose deaths has increased. And “opioid epidemic” when discussing overdoses highly obscures that heroin is the major contributor alongside fentanyl — not merely prescription analgesics. We hear a lot about OxyContin and Vicodin, which are actually leveling out (or were until 2015), and less about the drugs which are already policed more, have been policed longer, and cause more physical problems.
What the Commission proposes
In its report, the Commission concludes the goals of its recommendations are “to promote prevention of all drug use with effective education campaigns and restrictions in the supply of illicit and misused drugs.” The President’s Commission doesn’t want to interfere too strongly, despite all of Trump’s suggestions of a revamped drug war. The report notes that coming down hard on opioids will hurt patients with real needs, as has already happened, and, in a way, has happened since 1924. Much of the Commission’s recommendations come from a market approach, e.g. the suggestion (Rec. 19) to reimburse nonopioid pain treatments. The current Centers for Medicare and Medicaid Services (CMS) policy for reimbursement for healthcare providers treats nonopioid, postsurgical pain relief treatments the same as opioid prescriptions, issuing one inclusive payment for all “supplies” at a fixed fee. Nonopioid medications and treatments cost more, and so hospitals opt for dispensing opioids instead. The Commission recommends “adequate reimbursement [for] a broader range of pain management” services, changing the bundle payment policy to accommodate behavioral health treatment, educational programs, “tapering off opioids” and other nonopioid options.
Trump himself suggested an educational approach in a public announcement, which triggered critical comparisons to the failed D.A.R.E. program and “your brain on drugs” commercials. Educational programs are a less coercive option than direct regulation of opioids, but their effectiveness seems to be hit and miss. The Commission cites the Idaho Meth Project from 2007 (ongoing), conducted by a private nonprofit to inform young adults on the health problems associated with methamphetamine use, as a success story: “The Meth Project reports that 94% of teens that are aware of the anti-meth campaign ads say they make them less likely to try or use meth, and that Idaho has experienced a 56% decline in teen meth use since the campaign began.” This meth project is one success story out of many failures. For instance, the Montana Meth Project from 2005, on which the Idaho project was modelled, “accounting for a preexisting downward trend in meth use,” was determined to have “effects on meth use [that] are statistically indistinguishable from zero,” according to an analysis by the National Library of Medicine. Then again, one large scale anti-drug educational campaign, truth, which encourages youth to avoid tobacco, might be having success. Their modern guerrilla tactics are a major improvement on the old model of Partnership for a Drug-Free America.
In another market approach to help recovering addicts reenter society, the Commission recommends decoupling felony convictions and eligibility for certain occupations (Rec. 50). The report cites Section 1128 of the Social Security Act, which prohibits employers that receive funding from federal health programs from hiring past convicts charged with unlawfully manufacturing, distributing or dispensing controlled substances. Any confrontation with law enforcement is a barrier to landing a job — a protected area of discrimination — and government laws that specifically ban their hiring make it worse on ex-users and -dealers trying to get clean. Recommendations like these lessen the role that the state has in keeping ex-convicts out of work.
Much of the funding requested by the President’s Commission is authorized by the Obama administration’s major contribution to combating opioid usage, the Comprehensive Addiction and Recovery Act (CARA), signed into law July 2016 and credited as the “first major federal addiction legislation in 40 years.” CARA helped implement naloxone (an opioid overdose-reversal nail spray) in firefighting departments and strengthen drug monitoring programs.
I’ll post the second half soon, and then a bonus post on my personal favorite solution.
Midweek Reader: The Drug War, the Opioid Crisis, and the Moral Hazard of Overdose Treatment
Today, I’m reviving an old series I attempted to start last year that never came to fruition: The midweek reader. A micro-blogging series in which I try to link to stories that are related to each other to provide deeper insight into an issue. This week, we’re looking at the relationship between the Opioid Crisis and the drug war, and the academic debate around a controversial paper finding moral hazard in policies that try to increase access to Naloxone.
- At Harpers Magazine, Brian Gladstone has a fantastic long-form piece looking into how attempts to crack down on opioid addiction by targeting the prescription pain meds have left many patients behind and questioning the mainstream narrative that the rise of opioids was driven primarily by pain prescriptions. A slice:
Yet even the most basic elements of this disaster remain unclear. For while it’s true that the past three decades saw a staggering upsurge in the prescribing of opioid medication, this trend peaked in 2010 and has been declining since: high-dose prescriptions fell by 41 percent between 2010 and 2015. The question, then, is why overdose deaths continue to skyrocket, rising 37 percent over the same period — and whether restricting access to regulated drugs is actually pushing people toward more lethal, unregulated ones, such as fentanyl, heroin, and carfentanil, a synthetic opioid 10,000 times stronger than morphine.
- Similarly, at the Cato Institute, Jeffery A. Singer has a good piece exploring the relationship between America’s War on Drugs and the rise of opioid addictions. He concludes:
Meanwhile, President Trump and most state and local policymakers remain stuck on the misguided notion that the way to stem the overdose rate is to clamp down on the number and dose of opioids that doctors can prescribe to their patients in pain, and to curtail opioid production by the nation’s pharmaceutical manufacturers. And while patients are made to suffer needlessly as doctors, fearing a visit from a DEA agent, are cutting them off from relief, the overdose rate continues to climb.
- At Vox, philosopher Brendan de Kenessey of Harvard has a piece exploring the philosophy of the self and of rational choice to argue that it’s wrong to treat drug addiction as a moral failure. A slice:
We tend to view addiction as a moral failure because we are in the grip of a simple but misleading answer to one of the oldest questions of philosophy: Do people always do what they think is best? In other words, do our actions always reflect our beliefs and values? When someone with addiction chooses to take drugs, does this show us what she truly cares about — or might something more complicated be going on?
- An econometrics working paper by Jennifer L. Doleac of University of Virginia and Anita Mukherjee of the University of Wisconsin released earlier this month, which sparked spirited discussion, investigated the link between opioids and laws increasing access to Naloxone. They found the laws increased measurements of opioid use but did reduce mortality, which they theorize is because Naloxone increases moral hazard for addicts by reducing potential costs of an overdose. However, they conclude:
Our findings do not necessarily imply that we should stop making Naloxone available to individuals suffering from opioid addiction, or those who are at risk of overdose. They do imply that the public health community should acknowledge and prepare for the behavioral effects we find here. Our results show that broad Naloxone access may be limited in its ability to reduce the epidemic’s death toll because not only does it not address the root causes of addiction, but it may exacerbate them. Looking forward, our results suggest that Naloxone’s effects may depend on the availability of local drug treatment: when treatment is available to people who need help overcoming their addiction, broad Naloxone access results in more beneficial effects. Increasing access to drug treatment, then, might be a necessary complement to Naloxone access in curbing the opioid overdose epidemic.
- Alex Gertner, a PhD candidate at UNC-Chaple Hill, published a criticism of Doleac Murkhejee at Vox pointing out that their data linking Naloxone and opioid-related hospital visits are not necessarily due to a casual story involving moral hazard:
The authors find that naloxone access laws lead to more opioid-related emergency department visits, the premise being that naloxone access laws increase opioid overdoses. But there’s a far more likely explanation: People are generally instructed to seek medical care for overdose after receiving naloxone.
Overdose is a general term to describe experiencing the toxic effects of drugs. People can overdose, and often do, without either dying or seeking medical attention. If people who would otherwise overdose without medical attention are instead using naloxone and going to emergency rooms, that’s a good thing.
- The widest-ranging and most thorough critique of Doleac-Murkhejee comes from Frank, Pollack, and Humphries at the Journal of Health Affairs. They argue that the original authors (1) assume too much immediacy in effect of changes in Naloxone laws than is probably warranted (2) ignore a variety of exogenous variables like Medicare expansion. They conclude:
We believe the best interpretation of Doleac and Mukherjee’s findings is that their main treatment variable—naloxone laws—thus far have had little impact on naloxone use or nonmedical opioid use during the period studied. This disappointing pattern commands attention and follow-up from both public health practitioners and public health researchers.
Lunchtime Links
- High Hitler (drugs, drugs, drugs!)
- every generation gets the drugs it deserves
- Lawsplainer on federal and state marijuana laws
- why illegally obtained evidence is generally inadmissible in court
- Putin and patriotism: national pride after the fall of the Soviet Union (excerpt)
- long, fraught history of Pakistan and the US
- Old Dogs, New Tricks: Turkey and the Kurds
- Good piece, but I’m still waiting for a great book (or article) on the Hanseatic League. All the great ones are probably in German…
Vincent Geloso Interviewed for his Work on the War on Drugs
Regular readers of NOL know that fellow notewriter Vincent Geloso has done a lot of great work on the war on drugs. Dr. Geloso was recently on Student for Liberty’s Podcast to discuss a paper he recently co-authored compiling data on the effects of the war on drugs on increased security costs, which he previewed a few months ago on NOL. He had a wide-ranging discussion on his findings, secondary effects of the war on drugs in terms of economic costs, the psychology of policing with the war on drugs, and comparing the drug war to prohibition. Check out the discussion.
P.S. If you’re not already listening to SFL On Air, you should and not just because I’m in charge of marketing for it.
A hidden cost of the war on drugs
AI just completed another paper (this time with my longtime partner in crime Vadim Kufenko) where we question an hypothesis advanced by Samuel Bowles regarding the cost of inequality. In the process, we proposed an alternative explanation which has implications for the evaluation of the war on drugs.
In recent years, Samuel Bowles (2012) has advanced a theory (well-embedded within neoclassical theoretical elements while remaining elegantly simple) whereby inequality increases distrust which in turn magnifies agency problems. This forces firms to expend more resources on supervision and protection which means an expansion of the “guard labor force” (or supervisory labor force). Basically, he argues there is an over-provision of security and supervision. That is the cost of inequality which Bowles presents as a coordination failure. We propose an alternative explanation for the size of the guard and supervisory labor forces.
Our alternative is that there can be over-provision of security and supervision, but this could also be the result of a government failure. We argue that the war on drugs leads to institutional decay and lower levels of trust which, in turn, force private actors to deploy resources to supervise workers and protect themselves. Basically, efforts at prohibiting illicit substances require that limited policing resources be spread more thinly which may force private actors to expend more resources on security for themselves (thus creating an overprovision of security). This represents a form of state failure, especially if the attempts at policing these illicit substances increase the level of crime to which populations are vulnerable. To counteract this, private actors invest more in protection and supervision.
Using some of the work of Jeffrey Miron and Katherine Waldock, we show that increases in the intensity of prohibition enforcement efforts (measured in dollars per capita) have significant effects on the demand for guard labor. Given that guards represent roughly 1 million individuals in the US labor market, that is not a negligible outcome. We find that a one standard deviation increase in the level of drug enforcement efforts increases the ratio of guards to the population by somewhere between 12.92% and 13.91% (which is the equivalent of roughly 100,000 workers).
While our paper concentrated on proposing an alternative to the argument advanced by Bowles regarding the cost of inequality, we (more or less accidentally) measured a hidden cost from the war on drugs. The insecurity (increased crime rates and spillovers from illegal markets into formal markets) brought forth by drug prohibition forces an over-provision of security and supervision (our supervision measure which includes workers that supervise other workers were smaller than with the security guard measure).
Basically, a hidden (private cost) of the war on drugs is that we must reallocate resources that we could have used otherwise. Its a little like when I say that it is meaningless to compare healthcare expenditures to GDP in Canada and the United States because Canadians assume costs in a hidden manner through rationing. Waiting lists in Canada are longer than in the US. The cost is lost wages and enduring pain and that cost will not appear in measures of expenditures to GDP. The war on drugs works the same way. There is a fiscal cost (expenditures dedicated to it and the taxes that we must impose), there is a crime cost (destruction of lives and property) and there is a reallocation cost of privately providing security which is hard to measure.
The Enforcement Costs of Immigration Laws are Greater than Alleged Welfare Costs
As I mentioned in my note yesterday, the common argument that immigration is significantly costly through welfare is mostly empirically falsified. The fact of the matter is immigrants usually aren’t qualified for such programs, illegal immigrants mostly cannot and do not receive them, and immigrants as a whole wind up contributing more to the government’s balance sheet through economic growth and tax receipts than they take through welfare transfer payments.
However, there is one fact I neglected to mention yesterday worthy of its own post: if those opposed to immigration on the grounds of welfare costs were really sincere in that argument, they also need to consider the fiscal costs of enforcing their beloved immigration laws. As the New York Times editorial board pointed out yesterday, these costs are not insignificant:
The Migration Policy Institute reported in 2013 that the federal government spends more each year on immigration enforcement–through Immigration and Customs Enforcement and the Border Patrol–then on all other federal law enforcement agencies combined. The total has risen to more than $19 billion a year, and more than $306 billion in all since 1986, measured in 2016 dollars. This exceeds the sum of all spending for the Federal Bureau of Investigation; the Drug Enforcement Administration; the Secret Service; the Marshals Service; and the Bureau of Alcohol, Tobacco, Firearms, and Explosives.
These fiscal costs get worse when you consider that Donald Trump wants to expand ICE’s budget even further and, of course, the $8-$12 billion dollar wall.
Further, if you are a civil liberties type concerned with the social and fiscal costs of mass incarceration, immigration enforcement looks even bleaker:
ICE and the Border Patrol already refer more cases for federal prosecution than the entire Justice Department, and the number of people they detain each year (more than 400,000) is greater than the number of inmates being held by the Federal Bureau of Prisons for all other federal crimes.
The war on immigrants makes the war on drugs look tame.
Of course, these costs are pretty small when compared to the welfare state, but immigrants are not the ones driving up those welfare costs and they might even reduce it with more tax receipts. The truth is that furthering immigration restrictions and enforcement is truly fiscally irresponsible, not respecting the right to freedom of movement and contract.
So, something that makes me smile for a change.
It’s a fact that I feel pain in several parts of my body, including in parts I did not know I had. One of the sources of pain is permanent shingles. I only mention this in the hope that it will trigger some of you to get vaccinated or to get their aging parents vaccinated.
So, anyway, recently, someone who ought to know (if you know what I mean) convinced me to try cannabis for my pains. So, I went to the specialized doctor (at least, I think he is a doctor). I gave him $100 and I came out with a medical marijuana card.
I went straight to the dispensary and purchased some cookies, of the kind my adviser had previously let me taste. The effect on my pain was almost miraculous. I felt none from about five pm until I went to bed around 10 pm.
Several things sill trouble me. First, I can’t find a dose small enough to avoid getting a little high, which I would like to avoid. Second, it makes me hungry (surprise!). Third, what if frequent use re-ignites my passions, what then? Fourth, I am really, really pissed off about the $100 because it looks like Californians just passed a recreational cannabis law.
My sage adviser is an excellent auto mechanic in his spare time. You write me, I will give you his name. That would be for mechanical services, of course.
BC’s weekend reads
- Smuggling Nikita Khrushchev’s memoirs out of the USSR
- Are memes disrupting American politics? So asks a Leftist
- The 4th Amendment, policing, and pedagogy
- At least the end of the War on Drugs is nigh
- A new (old) strategy for a polycentric world (but why not federation?)
- A simple map of Brazil and its states
Another Race Riot
Note: This is written for my overseas readers mainly. If you live in the US, you will probably find that you already know most of what I am writing about.
A couple of days ago, a police officer shot to death a black man in full daylight in Charlotte, North Carolina, very much the Old South, former home of abject slavery.
This is happening in the last months of the second administration of the first black American president, after more than seven years of his being in charge. “Being in charge” is an exaggeration of sorts though. The President of the United States exercises no constitutional authority over local police forces (or state police forces). His federal Department of Justice only has jurisdiction when a violation of civil rights is at stake and only over that specific putative violation. Homicide is not in itself a civil rights violation. It’s true that Pres. Obama cannot pick up the phone and tell the Charlotte police what to do or how. Yet, Mr Obama is responsible to some extent although indirectly for the violence, an idea I will develop below.
Cop kills black man: familiar story, right?
I forgot to give you important information. The police officer who did the shooting is black and a woman. She answers to a black police chief. He is squarely in charge of training officers and making rules for their behavior, including their use of firearms. The Chief of Police is appointed and answers to the mayor of Charlotte. The mayor is a white woman and a prominent Democrat. She is assisted by a city council of eleven, four or whom are black. As far as I can tell, there are zero, or one, or two Republican city councilors. The rest are Democrats.
The police says the victim had a gun. His family says in was sitting in his car reading a book while waiting for his child to come out of school. Disturbingly different stories, for sure.
There have been three nights or protests in Charlotte, that quickly became riots, with demonstrators throwing heavy objects at police officers and much destruction of property. One demonstrator was shot, apparently not by a police officer. And, of course, there was much looting of stores. It’s nearly always like this: One young black man dies, fifteen young black men acquire brand new mountain bikes.
Watching the riots on TV, I notice something that television channels and printed press journalist don’t comment on: Some of the most aggressive rioters are young white men who seem to me to know what they are doing and who are not distracted by broken store windows. I should use the word cautiously but they seem to me almost professional in their approach to rioting. The white young rioters are not mentioned I think because they cannot be fitted in the prevailing liberal narrative: It’s a race riot, it’s a demonstration against racial injustice by black people who have just had enough. How about the young white guys? Irrelevant, they are just lovers of justice who happen to be there. Yet, I can’t claim that I recognize any of them on TV but there are young white men just like them in every race riot I have watched in the past two years. If they are absent the first day, they are plainly present the second day and the next few days.
The show on my TV looks a bit like a movie because it’s not well connected to reality, the reality that everyone knows: On the whole, young black men don’t die because cops shoot them, they die because other young black men kill them. They also kill the occasional child and lately, even a young mother pushing her baby carriage. The percentage of violent deaths of black men at police hands that are legally unjustified, must be minuscule. No one in Chicago demonstrates against this continuing mass killing by African-Americans. I think blacks and whites alike don’t because it would contradict the main, tired old liberal narrative: Injustice and racial oppression are the source of all evils in American society.
Young black men kill one another in gang wars for turf (for possession of a piece of ground.) The turf, the ground, is an important asset in the retail sale of illegal drugs. I would be curious of what would happen if Congress decriminalized all drug sales to adults and if a rational president signed the bill into law. I would bet that young black men’s death rate would plummet by 90% in a few weeks. I have no explanation as to why this is not done. It’s not as if the 40-year old so-called “War on Drugs” were working in reducing drug use!
After seven+ years of Obama, the economic gap between whites and blacks – however you measure it – has increased. African-Americans are worse off in relative terms than they were under Pres. Bush. This is no surprise to me. It’s a Democratic administration. The worst place for a black man to live in America is in Democratic-ruled big cities. It begins with Chicago, a Democratic city for 85 years. And then, there is Detroit, a war zone with no war. All this being said, we must not forget that most African-Americans lead lives that are both normal and peaceful, in crying contradiction to the narrative of continued racial oppression. There is a large minority of young black men however who have never had a job, who don’t look for one, who may have never known a person with a job except teachers and cops.
Democratic politicians have been promising salvation in the form of “social programs” paid for by those who do work. They have done so for fifty years. They have not implemented them, or the programs have done little good, or even worse. It’s time for a revolutionary new idea, one that’s very old, in fact. When there is rapid economic growth, employers compete for labor, even for the labor of the inexperienced, even for the labor of those usually seen as unemployable. Black Americans in ghettos need the same thing that all Americans need: vigorous and fast economic growth. This may be hard to believe but the United States has few problems that could not be solved by ten years of 3.5% annual GDP growth.
There is no sign of a search for economic development in the Democratic presidential candidate’s program. Donald Trump, by contrast, promises to reduce taxes and to rid business of many regulations. Historically, it’s usually enough to produce growth. Black Americans need less abstract “justice” and more of a fair chance. The left wing of the Democratic Party hates the very idea.

{kind=link}