In 1969, Colonel Luke Quinn, a U.S. Army Air Force officer in World War II, was diagnosed with inoperable gallbladder cancer. Surprisingly, he was referred to Dr. DeVita, the lymphoma specialist at National Cancer Institute, by the great Harvard pathologist Sidney Farber — famous for developing one of the most successful chemotherapies ever discovered. Nobody imagined back then that Colonel Luke Quinn, a wiry man with grey hair and a fierce frown with his unusual and likely incurable cancer, would significantly impact how we look at cancer as a disease.

Having been coerced to take up the case of Colonel Luke Quinn, despite gallbladder cancers not being his specialty, Dr.DeVita began to take a routine history, much to the annoyance of Luke Quinn who was used to being in command. Though Quinn glared at Dr.DeVita for reinitiating another agonizing round of (im)patient history, he said he had gone to his primary care physician in D.C. when his skin and the whites of his eyes had turned a deep shade of yellow — jaundice. Suspecting obstructive jaundice—a blockage somewhere in the gallbladder, Quinn was referred to Claude Welch, a famous abdominal surgeon at Mass general who had treated Pope John Paull II when he was shot in 1981. Instead of gallstones, the renowned surgeon found a tangled mass of tissue squeezing Quinn’s gallbladder—gallbladder cancer was pretty much a death sentence. On the pathologist’s confirmation, Quinn, being declared inoperable, was sent to Dr.DeVita at NCI as he wanted to be treated near his home.

Dr.DeVita, however, noticed something quite odd when he felt Quinn’s armpits during a routine examination. Quinn’s axillary lymph nodes—the cluster of glands working as a sentinel for what’s going on in the body—under his arms were enlarged and rubbery. These glands tend to become tender when the body has an infection and hard if it has solid tumors—like gallbladder cancer; they become rubbery if there is lymphoma. Being a lymphoma specialist, the startled Dr. DeVita questioned the possibility of a misdiagnosis—what if Quinn had lymphoma, not a solid tumor wrapping around his gallbladder leading to jaundice?
On being asked for his biopsy slides to be reevaluated, the always-in-command Colonel Luke Quinn angrily handed them over to the pathologist at NCI and sat impatiently in the waiting room. Costan Berard, the pathologist reviewing Quinn’s biopsy slides, detected an artifact in the image that had made it difficult to differentiate one kind of cancer cell from the other. Gallbladder cancers are elliptical, whereas Lymphoma cells are round. The roundish lymphoma cells can look like the elliptical gallbladder cancer cells when squeezed during the biopsy. This unusual finding by Berard explained why Quinn’s lymph nodes were not hard but rubbery. The new biopsy showed without a doubt that Quinn had non-Hodgkin’s lymphoma —the clumsy non-name we still go by to classify all lymphomas that are not Hodgkin’s disease.

The NCI was working on C-MOPP, a new cocktail of drugs to treat non-Hodgkin’s lymphoma that had shown a two-year remission in forty percent of aggressive versions of this disease. The always-in-command WW II veteran had somehow landed in the right place by accident! It was a long three months for the nurses though, as they hated him for leaning on the call button all-day, for complaining bitterly about the food, for chastising anyone who forgot to address him, Colonel Quinn, and for never thanking anyone. But incredibly, he was discharged without any sign of his tumor; he had gone from certain death to a fighting chance.
The fierce and unpleasant Colonel Quinn is crucial because his initial misdiagnosis unknowingly spurred the creation of a close network of influential people during his remarkable escape from certain death. He could do this because he was a friend and employee of the socialite and philanthropist Mary Lasker—the most consequential person in the politics of medical research. Read my earlier piece on her.

Mary Lasker, the timid, beehived socialite circumvented all conventions of medical research management and got the U.S. Congress to do things her way. Mary’s mantra was: Congress never funds a concept like “cancer research,” but propose funding an institute named after a feared disease, and Congress leaps on it. Her incessant lobbying with the backing of her husband, Albert Lasker and her confidante, Florence Mahoney, wife of the publisher of The Miami News, helped create the National Cancer Institute, the National Heart Institute, the National Eye Institute, the National Institute of Mental Health, the National Institute of Dental and Craniofacial Research, the National Institute of Arthritis and Metabolic Diseases, the National Institute of Aging, and the National Institute of Child Health and Human Development.

Though Mary Lasker knew the value of independent investigators pursuing their unique research interests, she supported projects only when a clinical goal was perceptible, like curing tuberculosis. In 1946, Mary, having noticed microbiologist Selman Waksman’s work on streptomycin—a new class of antibiotics effective against microbes resistant to penicillin—persuaded him and Merck pharmaceutical company to test the new drug against TB. By 1952 Mary’s instinct had won over Waksman’s initial skepticism as the widespread use of streptomycin halved the mortality from TB! Mary Lasker’s catalytic influence on basic research leading to a Nobel Prize-winning discovery is a case in point.
Her clout over Congress was in its prime through the 1950s and 60s when the National Cancer Institute (NCI) was developing the first cancer cures. It was also the period when Colonel Luke Quinn became her influential lieutenant. The Congress believed Luke Quinn represented the American Cancer Society, but he was Mary’s lobbyist in reality. When Quinn got sick, Mary used her contacts to get Welch and Sidney Farber, but it got her special attention when Quinn’s incurable torment was overcome. The ongoing public concern for cancer and Albert Lasker’s death due to pancreatic cancer made it an ideal disease for Mary to draw the battle lines. Quinn’s recovery convinced her that the necessary advance in basic research had occurred to justify taking the disease head-on. In April 1970, she began building bipartisan support by having the Senate create the National Panel of Consultants on the Conquest of Cancer. She prevailed over the Texas Democrat senator Ralph Yarborough to appoint her friend, a wealthy Republican businessman Benno C. Schmidt —the chairman of Memorial Sloan Kettering board of managers—to be the chairman on the conquest of cancer panel. She backed him up by arranging Sidney Farber as the co-chairman. The panel also included Colonel Luke Quinn and Mary herself.
In just six months, the panel issued “The Yarborough Report.” The report, mainly written by Colonel Luke Quinn and Mary Lasker, made far-reaching recommendations, including an independent national cancer authority. It recommended a substantial increase in funding for cancer research from $180 million in 1971 to $400 million in 1972 and reaching $1 billion by 1976. Finally, it recommended that the approval of anticancer drugs be moved from the FDA to the new cancer authority. Senator Edward Kennedy presented the recommendations as new legislation for the Ninety-Second Congress. Though not a Senate staff member, Colonel Quinn, trained by Mary in the art of testifying before the Congress, orchestrated the hearings, set the agenda, and selected the people who would testify.

The Nixon administration did not immediately embrace the bill as he wasn’t thrilled by Edward Kennedy’s involvement. Being Ted Kennedy’s close friend, Mary asked him to withdraw as a sponsor. Under Senator Pete Domenici, the bill renamed the National Cancer Act had to pass in the House. Paul Rogers, who headed the House Health subcommittee—Colonel Quinn and Mary Lasker had no influence over him—objected to removing the NCI from the NIH umbrella. He cautioned the NIH would face similar threats of separation in other disease areas. A revised bill agreed to this demand and kept the NCI under the NIH but gave it a separate budget and a director appointed by the President.
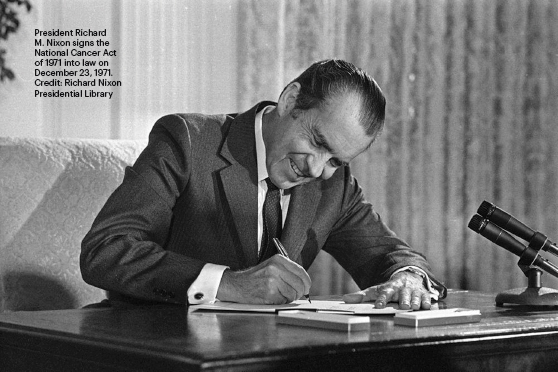
On December 23, 1971— fifty years to this day—the National Cancer Act was signed as a Christmas gift to the nation by President Richard Nixon, two years after Colonel Luke Quinn walked into the NCI with a wrong diagnosis. Though Quinn ultimately died of his relapsed cancer, a few months after the signing of the Cancer Act, the war on cancer had commenced with cancer research on the fast track. It was a victory for Mary Lasker, perhaps the most effective advocate for biomedical research that Washington had ever seen.

In hindsight, Mary Lasker’s triumph came with two significant disappointments. First, her crusade had failed in transferring the authority for approval of anticancer drugs from the FDA to the NCI—a failure that would plague the National Cancer Program well into the future. Second, the premise of the National Cancer Act that the “basic science was already there” and a quantitative boost in resources was all that was needed to bring victory was flawed. In combination, the two disappointments—the subjects of a future blog post—have spotlighted a perceived progress gap in cancer research by the tax-paying general public rather than underlining the tremendous conceptual progress made due to the War on Cancer.
Credit: National Cancer Institute / Univ. of Pittsburgh Cancer Institute
Ultimately, this blog is for you to appreciate the 50th anniversary of the lucky accidents and the incredible effort in creating the National Cancer Act. At the same time, personally, cancer researchers—the boots on the ground—like me who experience the non-triviality of progress in cancer will dwell on the insistence of simplistic linear views of progress in cancer research for public consumption.
