- Human crap Gabrielle Hecht, Aeon
- “So, as Lenin asked, what is to be done?” Howard Davies, Literary Review
- What the Democrats can learn from a dead libertarian lawyer Damon Root, Reason
- The Silk Road, the Black Death, and Covid-19 Parag Khanna, Wired
A PPE pandemic reading list
I haven’t written for a while – other duties get in the way – but I’d like to suggest this reading list in Philosophy, Politics, and Economics for the present time of crisis and perplexity. The main reason is that everyone seems to be an expert in Economics, Epidemiology, and Political Philosophy these days, assuming that from “facts” we can easily derive “values” and answer the question, “what is to be done?” I think this is at best a naïve attitude and at worst the same rationalistic hubris we experience everytime a political issue is simplified and reduced to a matter of “science”. Yes, there are facts and they shouldn’t be ignored, but it’s not easy to decide what is to be done, morally and politically, in light of those facts.
The first item on the list is Leviathan by Thomas Hobbes. A classic, and a reminder that people choose all the time to sacrifice some degree of liberty in the altar of survival (or a chance to survive), but also a reminder that Leviathan may turn from friend to foe, from protector to persecutor – and there is very little we can do about it. The second item is John Locke’s Second Treatise of Government, which then explores this topic in light of the fact that civil government shouldn’t have absolute power. It makes an attempt to show us how that power can, or should, be limited within a certain sphere of responsibility. Though it’s still there to protect us.
In this time of pandemic, people feel tempted to panic. People and politicians are calling for dramatic measures, and one reason is that the use of government coercion – which, according to Locke, ought to be limited – might be necessary to force people to cooperate, for example, by staying home. This is a proposed solution to the dilemmas of collective action posed by the problem that some may “free-ride” on the rest, and, as a result, the disease will keep spreading, frustrating any attempt to slow it down. Against dramatic, desperate and, perhaps, arrogant, use of political power, and in favor of prudence and wisdom, Edmund Burke’s collection of writings from the period of the French Revolution can be a beacon of light. On the other hand, explaining the dilemmas of collective action and suggesting ways of solving them, Mancur Olson offers an insightful look at incentives and group behavior in The Logic of Collective Action.
However, the idea that government coercion is the only solution to dilemmas of collective action (such as imposing a quarantine, for example) doesn’t hold water. In fact, other economists follow Olson in saying the problem is real and challenges a strict individualist way of thinking, but, adding to Olson’s point, they also acknowledge the role of private action and sanctions in fostering cooperation. Elinor Ostrom’s Governing the Commons is a wonderful study that opens up a number of possibilities for private enforcing of collective action to preserve and promote the frugal allocation of common goods. This can be complemented by The Quest for Community, an overlooked work by sociologist Robert Nisbet, where it becomes clear that, between individuals, the state, and the market, there’s room for other associations and communities that strengthen civil society – particularly in this challenging time. Nisbet’s lesson invites liberty-loving people to reflect on whether a hyper-individualistic view of the world ends up pitting helpess individuals against Leviathan instead of offering the buffer zone of community in between. This is something Alexis de Tocqueville discussed in the 19th century.
And just for the sake of dealing with the issue that “is” doesn’t easily lead to “ought”, and that science might have facts and an explanation for them, but does not easily conduce to a proper discussion on values policy, I must finish this PPE pandemic reading list with F. A. Hayek’s The Constitution of Liberty. On Chapter 4, for example, Hayek introduces a constrast between “rationalist liberalism” and “anti-rationalist liberalism”. Rationalist liberals assume too easily that knowledge of the facts on the ground will give them what they need to re-design a society governed by reason. Hayek warns us against this technocratic assumption and offers a defence of “anti-rationalist liberalism”. Anti-rationalist liberals understand the importance of spontaneous order and of constraining power (even at a time of crisis) while prudently balancing the values of liberty and safety in light of past experience and tradition.
Three Additional readings:
Buzan, Waever and De Wilde, Security: A New Framework for Analysis (1997). In a liberal democracy, the state steps in suspending some civil liberties only if it can persuade citizens that there’s a threat that justifies it. This book offers a framework to interpret how such threats are constructed in official and non-official discourse, and to what extent this construction of a threat can be effective.
Robert Higgs, Crisis and Leviathan (2013). 25th anniversary edition. Looks at US history and how government employed crises to its advantage and the advantage of the ruling elites. In particular, security and economy related issues are dealt with.
Sanford Ikeda, Dynamics of the Mixed Economy (2002). Shows that a time of crisis might be a time for further interventionism in the economy, as Higgs (see above) suggests, but might also be a time for disintervention, as seems to be the case with part of the agenda today (FDA deregulation, etc.) This is based on Ludwig von Mises’ view that interventionist economies are not very stable and are always swinging as a pendulum between socialism and capitalism.
The Vexing Libertarian Issue of Transition
I have appointed myself an old sage to the world. When your knees are creaky and every snotty eighteen-year-old treats you patronizingly, the least you can do to compensate is award yourself wisdom. Anyway, long story short, it’s a good excuse to spend much time on Facebook. I feel I am rendering a public service. I am continuing my teaching career there. It’s unpaid but the conditions are much better and all the students actually want to be in class.
Of course, it’s also true that Facebook is addictive. It’s not a bad addiction. For this old guy, it’s almost incredible to have frequent conversations with an MD in Pakistan, my niece in India, an old girlfriend in Panama, a young friend’s wife in Japan, and of course, many different kinds of French people. I even have a Facebook friend who lives in the mountains of Algeria; we have lively talks in French. Recently, a young woman who described herself as a Myanmar village girl reached out. (I know what you are thinking but if she is really one of those internet sex trolls, I salute the originality of her marketing strategy.) At all times a day and night, I have at least one Facebook friend who is not asleep. It’s pleasant in these days of confinement.
The same confinement, perhaps, slows me down and makes me more likely to tally up everything. As a result, a new impression has pierced my consciousness. Expressing contempt for democracy seems to be in vogue among people who identify as libertarians (with a small “l,” big “L” Libertarians have nearly vanished from my world. It could just be me.) This contempt reminds me that I have been asking the same question of libertarianism for now about fifty years, all with not much success.
I refer to the question of transition. I mean, what is it supposed to look like moving from wherever we are, in terms of governance, to a society with a drastically diminished government interference in individual lives? I have been receiving evasive answers, answers that don’t make even superficial sense, and swift escapes effected by changing the subject.
Let me say right away that I am not looking for a crushing reading assignment (a common punitive, passive-aggressive maneuver among intellectuals). Mine is a simple question. One should be able to sketch a rudimentary answer to it. Then, it would be up to me to follow through. Then, no excuse!
To my mind, there are only two extreme transition scenarios. One is the Somali scenario. The state falls apart under its own incapacity to limit internal aggression. It disappears or nearly so. When the point is reached where government authority extends only three blocks from the presidential palace to the north and east, and one block from the south and west, you pretty much have a stateless society. Goal reached!
The second scenario is a gradual change from the current “democratic” arrangements. I mean by this fair and reasonably honest elections followed by a peaceful transfer of power. I mean freedom of expression. And, disturbingly, this also includes courts of law. This is disturbing because courts without enforcement of their decisions are not really courts. This fact implies the threat of coercion, of course.
Now, I can imagine a situation like right now with the Corona Virus epidemic when governments (plural) demonstrate on a large scale their inability to do the obvious. The citizens often react to this sort of demonstration by asking for better and more government. However, it does not have to be that way. The combination of wide communication through the internet and – like now – of enforced leisure – may switch the dial. It’s conceivable that large numbers will get the idea that government that is at once heavy-handed, expensive, and incapable is not a good answer to much of anything. With that scenario one can imagine a collective demand for less government.
Strangely, this sort of scenario may be on display in France now, as I write. Well, this is not so strange after all. A deeply statist society where govt absorbs 55% of GDP and up may be exactly the best place to figure out that more government is not the answer. From this thought to the idea that less government may be the answer there is but one step. My intuition though is that it’s a big step. That’s because few people understand markets. No one but a handful of college professors seems to have read the moral philosopher Adam Smith. (Tell me that I am wrong.)
So, I would like for those who are more advanced than I am on this issue of transition (a low bar) to engage me. I am not interested in the same old ethical demonstrations though. Yes, the state is an instrument of coercion and therefore, evil. I already know this. In the meantime, the First Amendment to the Constitution of the United States does a fair job of protecting my freedom of speech, my freedom, of thought, my freedom of religion. I am not eager to leave this behind for the complete unknown. Are you? Why? How?
Nightcap
- The role of the libertarian in non-libertarian societies Fabio Rojas, Bleeding Heart Libertarians
- Did I have the coronavirus? Ross Douthat, New York Times
- Hospital bed access across Canada Frances Woolley, Worthwhile Canadian Initiative
- The future of public employee unions Daniel DiSalvo, National Affairs
A History of Plagues
As COVID-19 continues to spread, fears and extraordinary predictions have also gone viral. While facing a new infectious threat, the unknowns of how new traits of our societies worldwide or of this novel coronavirus impact its spread. Though no two pandemics are equivalent, I thought it best to face this new threat armed with knowledge from past infectious episodes. The best inoculation against a plague of panic is to use evidence gained through billions of deaths, thousands of years, and a few vital breakthroughs to prepare our knowledge of today’s biological crises, social prognosis, and choices.
Below, I address three key questions: First, what precedents do we have for infections with catastrophic potential across societies? Second, what are the greatest killers and how do pandemics compare? Lastly, what are our greatest accomplishments in fighting infectious diseases?
As foundation for understanding how threats like COVID-19 come about and how their hosts fight back, I recommend reading The Red Queen concerning the evolutionary impact and mechanisms of host-disease competition and listening to Sam Harris’ “The Plague Years” podcast with Matt McCarthy from August 2019, which predated COVID-19 but had a strangely prophetic discussion of in-hospital strategies to mitigate drug resistance and their direct relation to evolutionary competition.
- The Biggest Killers:
Infectious diseases plagued humanity throughout prehistory and history, with a dramatic decrease in the number of infectious disease deaths coming in the past 200 years. In 1900, the leading killers of people were (1) Influenza, (2) Tuberculosis, and (3) Intestinal diseases, whereas now we die from (1) Heart disease, (2) Cancer, and (3) Stroke, all chronic conditions. This graph shows not that humans have vanquished infectious disease as a threat, but that in the never-ending war of evolutionary one-upmanship, we have won battles consistently since 1920 forward. When paired with Jonathan Haidt’s Most Important Graph in the World, this vindicates humanity’s methods of scientific and economic progress toward human flourishing.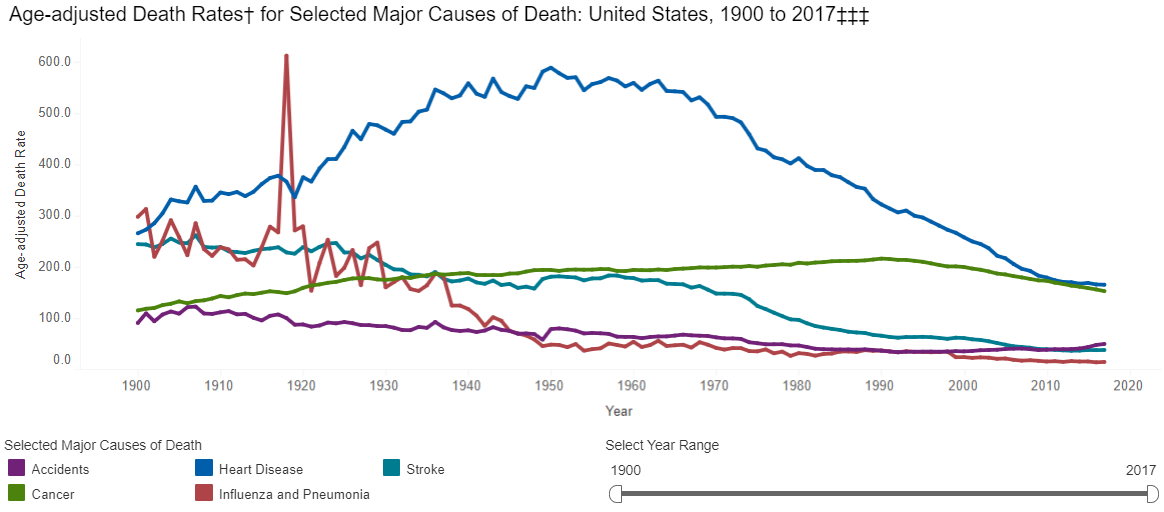
However, if the CDC had earlier data, it would show a huge range of diseases that dwarf wars and famines and dictators as causes of death in the premodern world. If we look to the history of plagues, we are really looking at the history of humanity’s greatest killers.
The sources on the history of pandemics are astonishingly sparse/non-comprehensive. I created the following graphs only by combining evidence and estimates from the WHO, CDC, Wikipedia, Our World in Data, VisualCapitalist, and others (lowest estimates shown where ranges were presented) for both major historic pandemics and for ongoing communicable disease threats. This is not a complete dataset, and I will continue to add to it, but it shows representative death counts from across major infectious disease episodes, as well as the death rate per year based on world population estimates. See the end of this post for the full underlying data. First, the top 12 “plagues” in history:
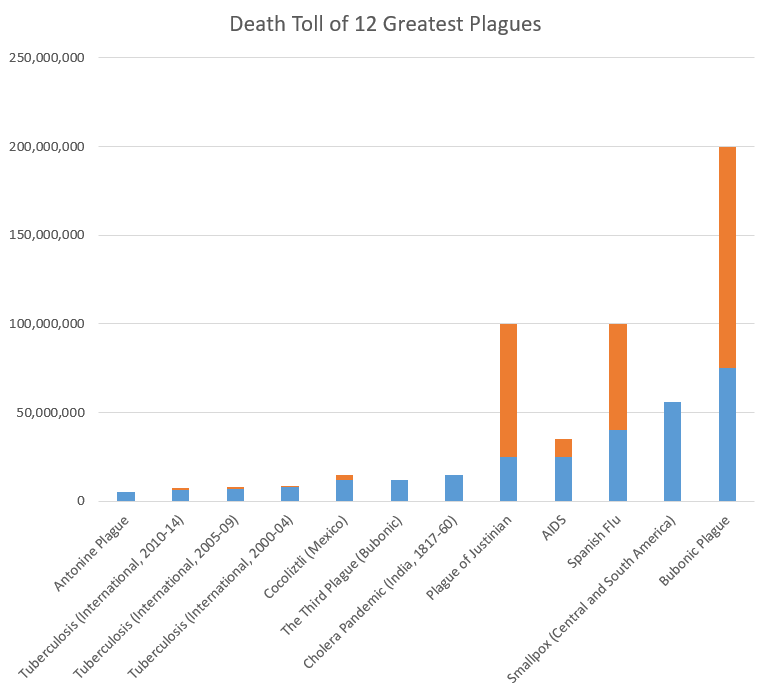
Note: blue=min, orange=max across the sources I examined. For ongoing diseases with year-by-year WHO evidence, like tuberculosis, measles, and cholera, I grouped mortality in 5-year spans (except AIDS, which does not have good estimates from the 1980s-90s, so I reported based on total estimated deaths).
Now, let’s look at the plagues that were lowest on my list (number 55-66). Again, my list was not comprehensive, but this should provide context for COVID-19:
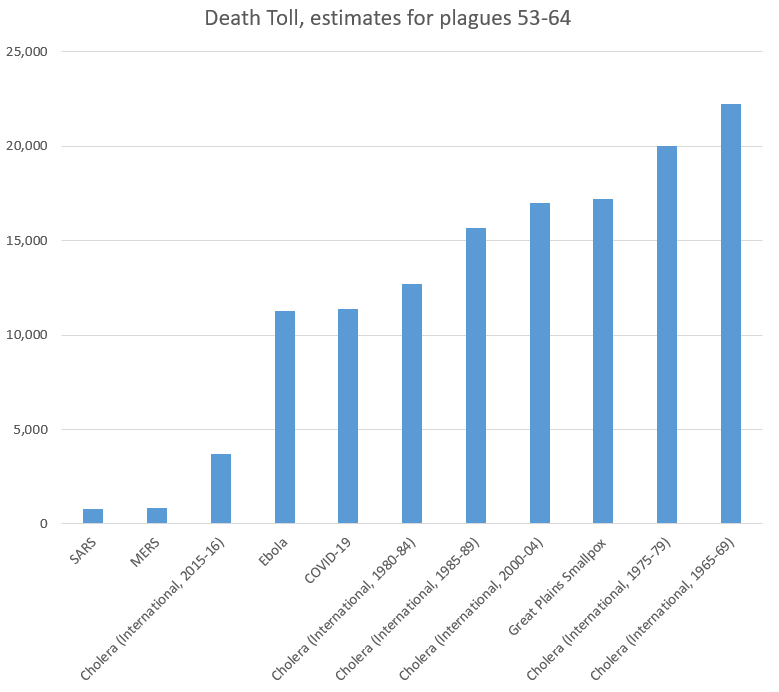
As we can see, the 11,400 people who have died from COVID-19 recently passed Ebola to take the 61st (out of 66) place on our list of plagues. Note again that several ongoing diseases were recorded in 5-year increments, and COVID-19 still comes in under the death rates for cholera. Even more notably, it has 0.015% as many victims as the plague in the 14th Century,
- In Context of Current Infectious Diseases:
For recent/ongoing diseases, it is easier to compare year-by-year data. Adding UNAIDS to our sources, we found the following rates of death across some of the leading infectious causes of death. Again, this is not comprehensive, but helps put COVID-19 (the small red dot, so far in the first 3 months of 2020) in context:
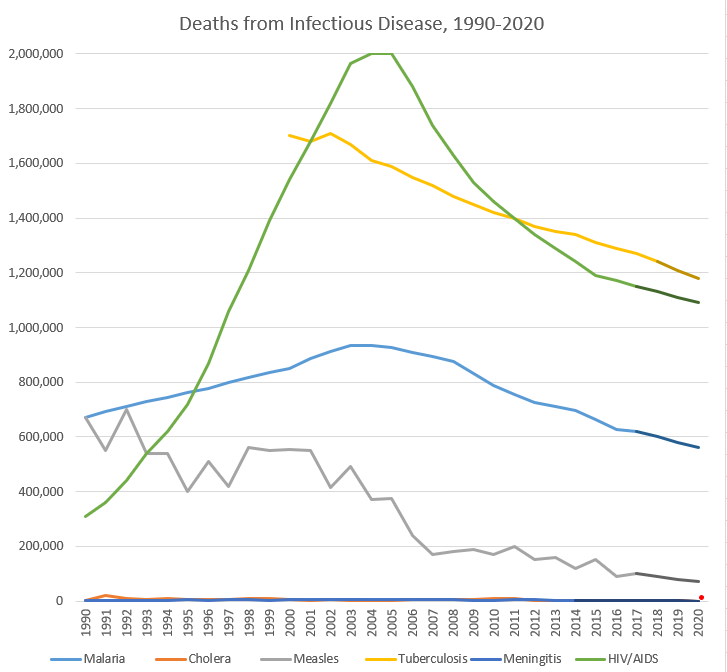
Note: darker segments of lines are my own estimates; full data at bottom of the post. I did not include influenza due to the lack of good sources on a year-by-year basis, but a Lancet article found that 291,000-645,000 deaths from influenza in a year is predictable based on data from 1999-2015.
None of this is to say that COVID-19 is not a major threat to human health globally–it is, and precautions could save lives. However, it should show us that there are major threats to human health globally all the time, that we must continue to fight. These trendlines tend to be going the right direction, but our war for survival has many foes, and will have more emerge in the future, and we should expend our resources in fighting them rationally based on the benefits to human health, not panic or headlines.
- The Eradication List:
As we think about the way to address COVID-19, we should keep in mind that this fight against infectious disease builds upon work so amazing that most internet junkies approach new infectious diseases with fear of the unknown, rather than tired acceptance that most humans succumb to them. That is a recent innovation in the human experience, and the strategies used to fight other diseases can inform our work now to reduce human suffering.
While influenzas may be impossible to eradicate (in part due to an evolved strategy of constantly changing antigens), I wanted to direct everyone to an ever-growing monument to human achievement, the Eradication List. While humans have eradicated only a few infectious diseases, the amazing thing is that we can discuss which diseases may in fact disappear as threats through the work of scientists.
On that happy note, I leave you here. More History of Plagues to come, in Volume 2: Vectors, Vaccines, and Virulence!
| Disease | Start Year | End Year | Death Toll (low) | Death Toll (high) | Deaths per 100,000 people per year (global) |
| Antonine Plague | 165 | 180 | 5,000,000 | 5,000,000 | 164.5 |
| Plague of Justinian | 541 | 542 | 25,000,000 | 100,000,000 | 6,250.0 |
| Japanese Smallpox Epidemic | 735 | 737 | 1,000,000 | 1,000,000 | 158.7 |
| Bubonic Plague | 1347 | 1351 | 75,000,000 | 200,000,000 | 4,166.7 |
| Smallpox (Central and South America) | 1520 | 1591 | 56,000,000 | 56,000,000 | 172.8 |
| Cocoliztli (Mexico) | 1545 | 1545 | 12,000,000 | 15,000,000 | 2,666.7 |
| Cocoliztli resurgence (Mexico) | 1576 | 1576 | 2,000,000 | 2,000,000 | 444.4 |
| 17th Century Plagues | 1600 | 1699 | 3,000,000 | 3,000,000 | 6.0 |
| 18th Century Plagues | 1700 | 1799 | 600,000 | 600,000 | 1.0 |
| New World Measles | 1700 | 1799 | 2,000,000 | 2,000,000 | 3.3 |
| Smallpox (North America) | 1763 | 1782 | 400,000 | 500,000 | 2.6 |
| Cholera Pandemic (India, 1817-60) | 1817 | 1860 | 15,000,000 | 15,000,000 | 34.1 |
| Cholera Pandemic (International, 1824-37) | 1824 | 1837 | 305,000 | 305,000 | 2.2 |
| Great Plains Smallpox | 1837 | 1837 | 17,200 | 17,200 | 1.7 |
| Cholera Pandemic (International, 1846-60) | 1846 | 1860 | 1,488,000 | 1,488,000 | 8.3 |
| Hawaiian Plagues | 1848 | 1849 | 40,000 | 40,000 | 1.7 |
| Yellow Fever | 1850 | 1899 | 100,000 | 150,000 | 0.2 |
| The Third Plague (Bubonic) | 1855 | 1855 | 12,000,000 | 12,000,000 | 1,000.0 |
| Cholera Pandemic (International, 1863-75) | 1863 | 1875 | 170,000 | 170,000 | 1.1 |
| Indian Smallpox | 1868 | 1907 | 4,700,000 | 4,700,000 | 9.8 |
| Franco-Prussian Smallpox | 1870 | 1875 | 500,000 | 500,000 | 6.9 |
| Cholera Pandemic (International, 1881-96) | 1881 | 1896 | 846,000 | 846,000 | 4.4 |
| Russian Flu | 1889 | 1890 | 1,000,000 | 1,000,000 | 41.7 |
| Cholera Pandemic (India and Russia) | 1899 | 1923 | 1,300,000 | 1,300,000 | 3.3 |
| Cholera Pandemic (Philippenes) | 1902 | 1904 | 200,000 | 200,000 | 4.2 |
| Spanish Flu | 1918 | 1919 | 40,000,000 | 100,000,000 | 1,250.0 |
| Cholera (International, 1950-54) | 1950 | 1954 | 316,201 | 316,201 | 2.4 |
| Cholera (International, 1955-59) | 1955 | 1959 | 186,055 | 186,055 | 1.3 |
| Asian Flu | 1957 | 1958 | 1,100,000 | 1,100,000 | 19.1 |
| Cholera (International, 1960-64) | 1960 | 1964 | 110,449 | 110,449 | 0.7 |
| Cholera (International, 1965-69) | 1965 | 1969 | 22,244 | 22,244 | 0.1 |
| Hong Kong Flu | 1968 | 1970 | 1,000,000 | 1,000,000 | 9.4 |
| Cholera (International, 1970-75) | 1970 | 1974 | 62,053 | 62,053 | 0.3 |
| Cholera (International, 1975-79) | 1975 | 1979 | 20,038 | 20,038 | 0.1 |
| Cholera (International, 1980-84) | 1980 | 1984 | 12,714 | 12,714 | 0.1 |
| AIDS | 1981 | 2020 | 25,000,000 | 35,000,000 | 13.8 |
| Measles (International, 1985) | 1985 | 1989 | 4,800,000 | 4,800,000 | 19.7 |
| Cholera (International, 1985-89) | 1985 | 1989 | 15,655 | 15,655 | 0.1 |
| Measles (International, 1990-94) | 1990 | 1994 | 2,900,000 | 2,900,000 | 10.9 |
| Cholera (International, 1990-94) | 1990 | 1994 | 47,829 | 47,829 | 0.2 |
| Malaria (International, 1990-94) | 1990 | 1994 | 3,549,921 | 3,549,921 | 13.3 |
| Measles (International, 1995-99) | 1995 | 1999 | 2,400,000 | 2,400,000 | 8.4 |
| Cholera (International, 1995-99) | 1995 | 1999 | 37,887 | 37,887 | 0.1 |
| Malaria (International, 1995-99) | 1995 | 1999 | 3,987,145 | 3,987,145 | 13.9 |
| Measles (International, 2000-04) | 2000 | 2004 | 2,300,000 | 2,300,000 | 7.5 |
| Malaria (International, 2000-04) | 2000 | 2004 | 4,516,664 | 4,516,664 | 14.7 |
| Tuberculosis (International, 2000-04) | 2000 | 2004 | 7,890,000 | 8,890,000 | 25.7 |
| Cholera (International, 2000-04) | 2000 | 2004 | 16,969 | 16,969 | 0.1 |
| SARS | 2002 | 2003 | 770 | 770 | 0.0 |
| Measles (International, 2005-09) | 2005 | 2009 | 1,300,000 | 1,300,000 | 4.0 |
| Malaria (International, 2005-09) | 2005 | 2009 | 4,438,106 | 4,438,106 | 13.6 |
| Tuberculosis (International, 2005-09) | 2005 | 2009 | 7,210,000 | 8,010,000 | 22.0 |
| Cholera (International, 2005-09) | 2005 | 2009 | 22,694 | 22,694 | 0.1 |
| Swine Flu | 2009 | 2010 | 200,000 | 500,000 | 1.5 |
| Measles (International, 2010-14) | 2010 | 2014 | 700,000 | 700,000 | 2.0 |
| Malaria (International, 2010-14) | 2010 | 2014 | 3,674,781 | 3,674,781 | 10.6 |
| Tuberculosis (International, 2010-14) | 2010 | 2014 | 6,480,000 | 7,250,000 | 18.6 |
| Cholera (International, 2010-14) | 2010 | 2014 | 22,691 | 22,691 | 0.1 |
| MERS | 2012 | 2020 | 850 | 850 | 0.0 |
| Ebola | 2014 | 2016 | 11,300 | 11,300 | 0.1 |
| Malaria (International, 2015-17) | 2015 | 2017 | 1,907,872 | 1,907,872 | 8.6 |
| Tuberculosis (International, 2015-18) | 2015 | 2018 | 4,800,000 | 5,440,000 | 16.3 |
| Cholera (International, 2015-16) | 2015 | 2016 | 3,724 | 3,724 | 0.0 |
| Measles (International, 2019) | 2019 | 2019 | 140,000 | 140,000 | 1.8 |
| COVID-19 | 2019 | 2020 | 11,400 | 11,400 | 0.1 |
| Year | Malaria | Cholera | Measles | Tuberculosis | Meningitis | HIV/AIDS | COVID-19 |
| 1990 | 672,518 | 2,487 | 670,000 | 1,903 | 310,000 | ||
| 1991 | 692,990 | 19,302 | 550,000 | 1,777 | 360,000 | ||
| 1992 | 711,535 | 8,214 | 700,000 | 2,482 | 440,000 | ||
| 1993 | 729,735 | 6,761 | 540,000 | 1,986 | 540,000 | ||
| 1994 | 743,143 | 10,750 | 540,000 | 3,335 | 620,000 | ||
| 1995 | 761,617 | 5,045 | 400,000 | 4,787 | 720,000 | ||
| 1996 | 777,012 | 6,418 | 510,000 | 3,325 | 870,000 | ||
| 1997 | 797,091 | 6,371 | 420,000 | 5,254 | 1,060,000 | ||
| 1998 | 816,733 | 10,832 | 560,000 | 4,929 | 1,210,000 | ||
| 1999 | 834,692 | 9,221 | 550,000 | 2,705 | 1,390,000 | ||
| 2000 | 851,785 | 5,269 | 555,000 | 1,700,000 | 4,298 | 1,540,000 | |
| 2001 | 885,057 | 2,897 | 550,000 | 1,680,000 | 6,398 | 1,680,000 | |
| 2002 | 911,230 | 4,564 | 415,000 | 1,710,000 | 6,122 | 1,820,000 | |
| 2003 | 934,048 | 1,894 | 490,000 | 1,670,000 | 7,441 | 1,965,000 | |
| 2004 | 934,544 | 2,345 | 370,000 | 1,610,000 | 6,428 | 2,003,000 | |
| 2005 | 927,109 | 2,272 | 375,000 | 1,590,000 | 6,671 | 2,000,000 | |
| 2006 | 909,899 | 6,300 | 240,000 | 1,550,000 | 4,720 | 1,880,000 | |
| 2007 | 895,528 | 4,033 | 170,000 | 1,520,000 | 7,028 | 1,740,000 | |
| 2008 | 874,087 | 5,143 | 180,000 | 1,480,000 | 4,363 | 1,630,000 | |
| 2009 | 831,483 | 4,946 | 190,000 | 1,450,000 | 3,187 | 1,530,000 | |
| 2010 | 788,442 | 7,543 | 170,000 | 1,420,000 | 2,198 | 1,460,000 | |
| 2011 | 755,544 | 7,781 | 200,000 | 1,400,000 | 3,726 | 1,400,000 | |
| 2012 | 725,676 | 3,034 | 150,000 | 1,370,000 | 3,926 | 1,340,000 | |
| 2013 | 710,114 | 2,102 | 160,000 | 1,350,000 | 3,453 | 1,290,000 | |
| 2014 | 695,005 | 2,231 | 120,000 | 1,340,000 | 2,992 | 1,240,000 | |
| 2015 | 662,164 | 1,304 | 150,000 | 1,310,000 | 1,190,000 | ||
| 2016 | 625,883 | 2,420 | 90,000 | 1,290,000 | 1,170,000 | ||
| 2017 | 619,825 | 100,000 | 1,270,000 | 1,150,000 | |||
| 2018 | 1,240,000 | ||||||
| 2019 | |||||||
| 2020 | 16,514 |
Nightcap
- The Old Normal Andrew Bacevich, Harper’s
- “Iran Doesn’t Want War but has a big appetite for risk” War on the Rocks
- Nice try, economists Arnold Kling, askblog
- Against “aggregate demand” Chris Dillow, Stumbling and Mumbling
Pandemic responses are beyond Evidence-based Medicine
John Ioannidis, a professor of medicine at Stanford University, fears that the draconian measures to enforce social distancing across Europe and United States could end up causing more harm than the pandemic itself. He believes that governments are acting on exaggerated claims and incomplete data and that a priority must be getting a more representative sample of populations currently suffering corona infections. I agree additional data would be enormously valuable but, following Saloni Dattani, I think we have more warrant for strong measures than Ioannidis implies.
Like Ioannidis’ Stanford colleague Richard Epstein, I agree that estimates of a relatively small overall fatality rate are plausible projections for most of the developed world and especially the United States. Unlike Epstein, I think those estimates are conditional on the radical social distancing (and self-isolation) measures that are currently being pushed rather than something that can be assumed. I am not in a position to challenge Ioannidis’ understanding of epidemiology. Others have used his piece as an opportunity to test and defend the assumptions of the worst-case scenarios.
Nevertheless, I can highlight the epistemic assumptions underlying Ioannidis’ pessimism about social distancing interventions. Ioannidis is a famous proponent (occasionally critic) of Evidence-based Medicine (EBM). Although open to refinement, at its core EBM argues that strict experimental methods (especially randomized controlled trials) and systematic reviews of published experimental studies with sound protocols are required to provide firm evidence for the success of a medical intervention.
The EBM movement was born out of a deep concern of its founder, Archie Cochrane, that clinicians wasted scarce resources on treatments that were often actively harmful for patients. Cochrane was particularly concerned that doctors could be dazzled or manipulated into using a treatment based on some theorized mechanism that had not been subject to rigorous testing. Only randomized controlled trials supposedly prove that an intervention works because only they minimize the possibility of a biased result (where characteristics of a patient or treatment path other than the intervention itself have influenced the result).
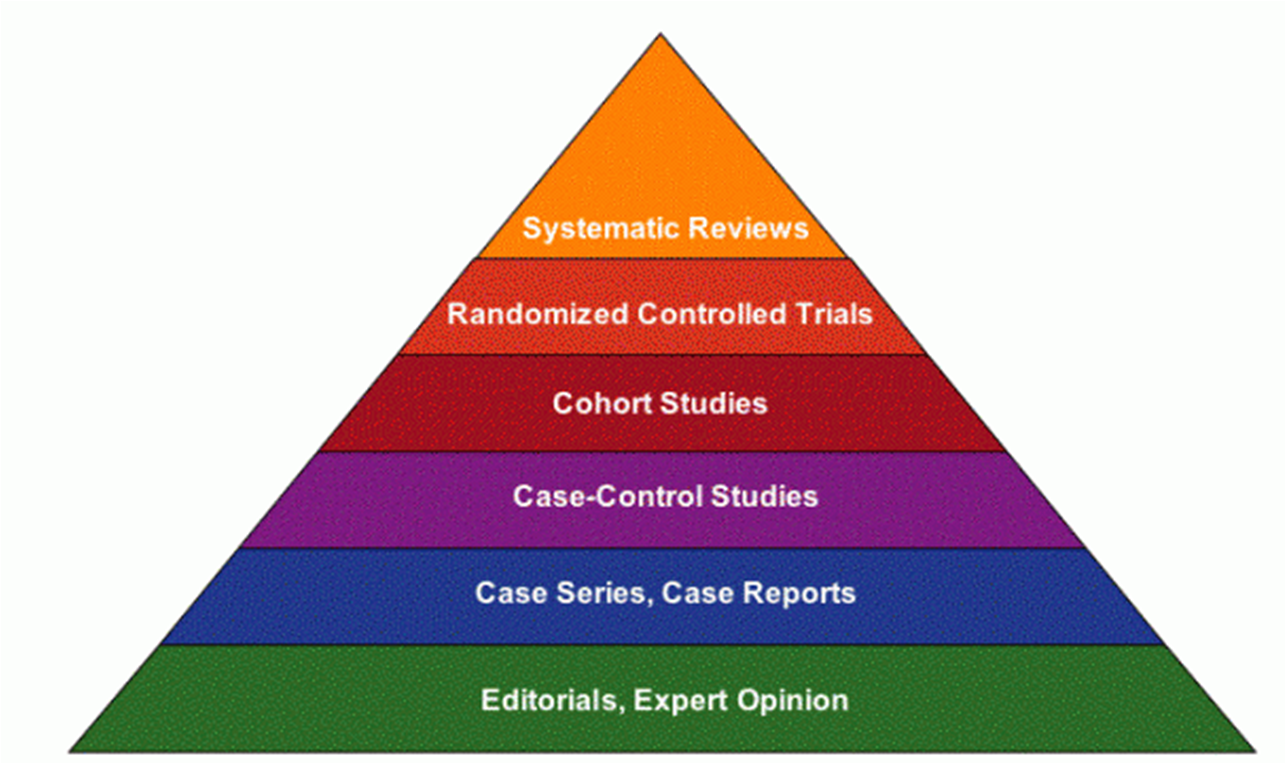
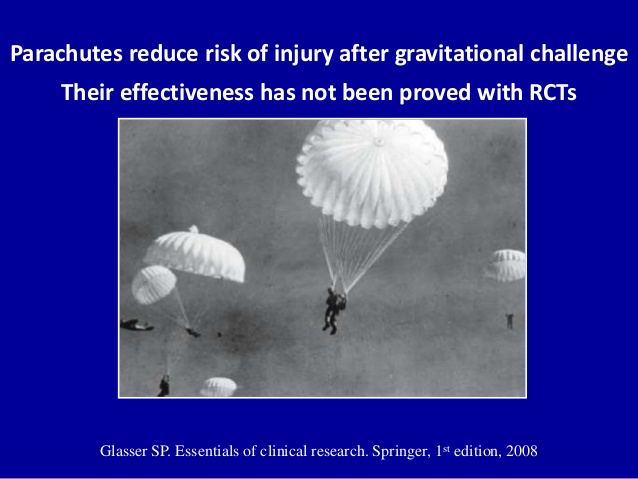
So when Ioannidis looks for evidence that social distancing interventions work, he reaches for a Cochrane Review that emphasizes experimental studies over other research designs. As is often the case for a Cochrane review, many of the results point to uncertainty or relatively small effects from the existing literature. But is this because social distancing doesn’t work, or because RCTs are bad at measuring their effectiveness under pandemic circumstances (the circumstances where they might actually count)? The classic rejoinder to EBM proponents is that we know that parachutes can save lives but we can never subject them to RCT. Effective pandemic interventions could suffer similar problems.
Nancy Cartwright and I have argued that there are flaws in the methodology underlying EBM. A positive result for treatment against control in a randomized controlled trial shows you that an intervention worked in one place, at one time for one set of patients but not why and whether to expect it to work again in a different context. EBM proponents try to solve this problem by synthesizing the results of RCTs from many different contexts, often to derive some average effect size that makes a treatment expected to work overall or typically. The problem is that, without background knowledge of what determined the effect of an intervention, there is little warrant to be confident that this average effect will apply in new circumstances. Without understanding the mechanism of action, or what we call a theory of change, such inferences rely purely on induction.
The opposite problem is also present. An intervention that works for some specific people or in some specific circumstances might look unpromising when it is tested in a variety of cases where it does not work. It might not work ‘on average’. But that does not mean it is ineffective when the mechanism is fit to solve a particular problem such as a pandemic situation. Insistence on a narrow notion of evidence will mean missing these interventions in favor of ones that work marginally in a broad range of cases where the answer is not as important or relevant.
Thus even high-quality experimental evidence needs to be combined with strong background scientific and social scientific knowledge established using a variety of research approaches. Sometimes an RCT is useful to clinch the case for a particular intervention. But sometimes, other sources of information (especially when time is of the essence), can make the case more strongly than a putative RCT can.
In the case of pandemics, there are several reasons to hold back from making RCTs (and study designs that try to imitate them) decisive or required for testing social policy:
- There is no clear boundary between treatment and control groups since, by definition, an infectious disease can spread between and influence groups unless they are artificially segregated (rendering the experiment less useful for making broader inferences).
- The outcome of interest is not for an individual patient but the communal spread of a disease that is fatal to some. The worst-case outcome is not one death, but potentially very many deaths caused by the chain of infection. A marginal intervention at the individual level might be dramatically effective in terms of community outcomes.
- At least some people will behave differently, and be more willing to alter their conduct, during a widely publicized pandemic compared to hygienic interventions during ordinary times. Although this principle might be testable in different circumstances, the actual intervention won’t be known until it is tried in the reality of pandemic.
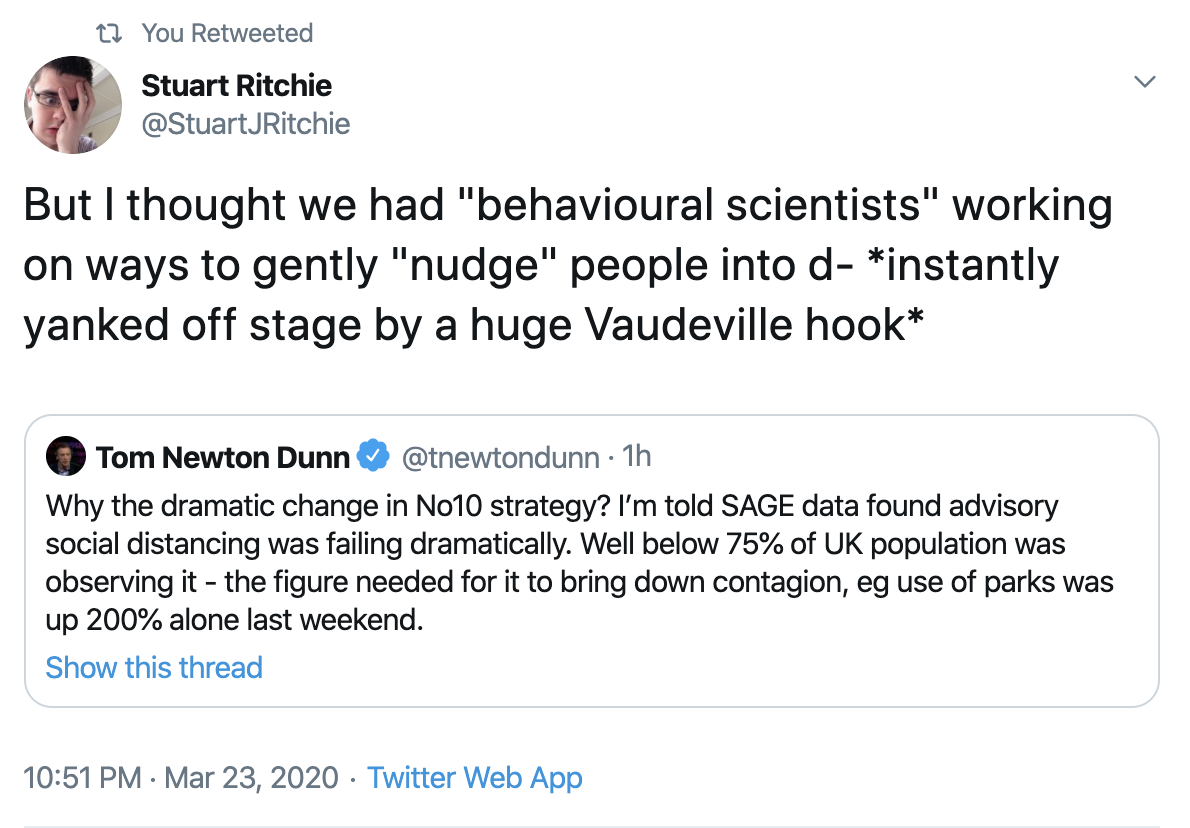
This means that rather than narrowly focusing on evidence from EBM and behavioral psychologists (or ‘nudge’), policymakers responding to pandemics must look to insights from political economy and social psychology, especially how to shift norms towards greater hygiene and social distancing. Without any bright ideas, traditional public health methods of clear guidance and occasionally enforced sanctions are having some effect.
What evidence do we have at the moment? Right now, there is an increasing body of defeasible knowledge of the mechanisms with which the Coronavirus spreads. Our knowledge of existing viruses with comparable characteristics indicates that effectively implemented social distancing is expected to slow its spread and that things like face masks might slow the spread when physical distancing isn’t possible.
We also have some country and city-level policy studies. We saw an exponential growth of cases in China before extreme measures brought the virus under control. We saw immediate quarantine and contact tracing of cases in Singapore and South Korea that was effective without further draconian measures but required excellent public health infrastructure.
We have now also seen what looks like exponential growth in Italy, followed by a lockdown that appears to have slowed the growth of cases though not yet deaths. Some commentators do not believe that Italy is a relevant case for forecasting other countries. Was exponential growth a normal feature of the virus, or something specific to Italy and its aging population that might not be repeated in other parts of Europe? This seems like an odd claim at this stage given China’s similar experience. The nature of case studies is that we do not know with certainty what all the factors are while they are in progress. We are about to learn more as some countries have chosen a more relaxed policy.
Is there an ‘evidence-based’ approach to fighting the Coronavirus? As it is so new: no. This means policymakers must rely on epistemic practices that are more defeasible than the scientific evidence that we are used to hearing. But that does not mean a default to light-touch intervention is prudent during a pandemic response. Instead, the approaches that use models with reasonable assumptions based on evidence from unfolding case-studies are the best we can do. Right now, I think, given my moral commitments, this suggests policymakers should err on the side of caution, physical distancing, and isolation while medical treatments are tested.
[slightly edited to distinguish my personal position from my epistemic standpoint]
Nightcap
- Rand Paul tests positive for coronavirus Bresnahan & Ferris, Politico
- The urgent lessons of World War I Brian Frydenborg, Modern War Institute
- Underestimating China Scott Sumner, MoneyIllusion
- Albania was not a True Communist country during the Cold War Griselda Qosja, Jacobin
Coronavirus and the BRI
The Corona Virus epidemic has shaken the world in numerous ways. The virus, which first emerged in the Chinese city of Wuhan (Hubei province), has led to the loss of over 12,000 lives globally. The three countries most impacted so far have been Italy (4,825 lives lost), China (3,287 lives lost), and Iran (1,500 lives lost) as of Saturday, March 21, 2020.
While there are reports that China is limping back to normalcy, the overall outlook for the economy is grim, to say the least, with some forecasts clearly predicting that even with aggressive stimulus measures China may not be able to attain 3% growth this year.
The Chinese slow down could have an impact on the country’s ambitious Belt and Road Initiative (BRI). While China has been trying to send out a message that BRI will not be impacted excessively, the ground realities could be different given a number of factors.
One of the important, and more controversial, components of the BRI has been the $62 billion China Pakistan Economic Corridor (CPEC), which has often been cited as a clear indicator of ‘Debt Trap Diplomacy’ (this, some analysts argue, is China’s way of increasing other country’s dependency on it, by providing loans for big ticket infrastructural projects, which ultimately lead to a rise in debts).
The US and multilateral organizations like the International Monetary Fund (IMF) have predictably questioned the project, but even in Pakistan many have questioned CPEC, including politicians, with most concerns revolving around its transparency and long-term economic implications. Yet the Imran Khan-led Pakistan Tehreek-E-Insaaf (PTI) government, and the previous Pakistan Muslim League (Nawaz) (PML-N) government, have given the project immense importance, arguing that it would be a game changer for the South Asian nation.
On more than one occasion, Beijing has assured Pakistan that CPEC will go ahead as planned with China’s Ambassador to Pakistan, Yao Jing, stating on numerous occasions that the project will not be hit in spite of the Corona Virus. Senior officials in the Imran Khan government, including the Railway Minister Sheikh Rashid Ahmed and Foreign Minister Shah Mehmood Qureshi, in an interview with the Global Times, stated that while in the short run Corona may have an impact on CPEC, in the long run there would be no significant impact.
Analysts in Pakistan however, doubt that there will be no impact, given the fact that a large number of Chinese workers who had left Pakistan are unlikely to return. Since February 2020, a number of reports have been predicting that the CPEC project is likely to be impacted significantly.
Similarly, in the cases of other countries too, there are likely to be significant problems with regard to the resource crunch in China as well as the fact that Chinese workers cannot travel. Not only is Beijing not in a position to send workers, but countries hit by COVID-19 themselves will not be in a position to get the project back on track immediately, as they will first have to deal with the consequences of the outbreak.
Some BRI projects which had begun to slow down even before the outbreak spread globally were in Indonesia and Bangladesh. In Indonesia, a high speed rail project connecting Jakarta with Bandung (estimated at $6 billion) has slowed down since the beginning of the year, and ever since the onset of the Corona Virus, skilled Chinese personnel have been prevented from going back to Indonesia. Bangladesh too has announced delays on the Payra Coal power plant in February 2020. As casualties arising out of the virus increase in Indonesia and other parts of Asia and Africa, the first priority for countries is to prevent the spread of the virus.
While it is true that Beijing would want to send a clear message of keeping its commitments, matching up to its earlier targets is not likely to be a mean task. Even before the outbreak, there were issues due to the terms and conditions of the project and a number of projects had to be renegotiated due to pressure from local populations.
What China has managed to do successfully is provide assistance for dealing with COVID-19. In response to a request for assistance from the Italian government, China has sent a group of 300 doctors and corona virus testing kits and ventilators. The founder of Ali Baba and one of Asia’s richest men, Jack Ma, has also taken the lead in providing assistance to countries in need. After announcing that he will send 500,000 coronavirus testing kits and 1 million masks to the United States, Ma pledged to donate more than 1 million kits to Africa on Monday March 17, 2020, and on March 21, 2020, in a tweet, the Chinese billionaire said that he would be donating emergency supplies to a number of South Asian and South East Asian countries — Afghanistan, Bangladesh, Cambodia, Laos, Maldives, Mongolia, Myanmar, Nepal, Pakistan, and Sri Lanka. The emergency supplies include 1.8 million masks, 210,000 test kits, 36,000 protective suits and ventilators, and thermometers.
China is bothered not just about it’s own economic gains from the BRI, but is also concerned about the long term interests of countries which have signed up for BRI.
The Corona Virus has shaken the whole world, not just China, and the immediate priority of most countries is to control the spread of the pandemic and minimize the number of casualties. Countries dependent upon China, especially those which have joined the BRI, are likely to be impacted. What remains to be seen is the degree to which BRI is affected, and how developing countries which have put high stakes on BRI related projects respond.
Nightcap
- Four types of labor and the epidemic Branko Milanovic, globalinequality
- Republicans, Democrats, and coronavirus Ronald Brownstein, Atlantic
- War with Iran: Regrets only Irfan Khawaja, Policy of Truth
- Taiwan’s robust constitutionalism and coronavirus Wen-Chen Chang, Verfassungsblog
Nightcap
- Keith Hart (economic anthropologist), RIP Cultural Anthropology
- Do you feel lucky, punk? Robin Hanson, Overcoming Bias
- From nation-states to interstellar civilization Nick Nielsen, Grand Strategy Annex
- “Under the Virus’s Cloak, Trump Pursues Long-Sought Policies” NYT
Nightcap
- The Use of Knowledge in Society F.A. Hayek, American Economic Review
- On conservative nationalism and foreign policy Emma Ashford, War on the Rocks
- Europe’s ‘solidarity’ crumbles in the face of a crisis Kai Weiss, CapX
- Bigger Brother: surveillance capitalism Tim Wu, New York Review of Books
Never reason from a fatality rate
Richard Epstein has produced several posts and a video interview arguing that the mainstream media is overreacting to the Coronavirus pandemic. Richard understands the potential seriousness of this situation and the proper role of government. He recognises the value of the Roman maxim Salus populi suprema lex esto – let the health of the people be the highest law. In public health emergencies, many moral and legal claims resulting from individual rights and contracts are vitiated, and some civil liberties suspended.
Nevertheless, along with Cass Sunstein, Richard claims that this particular emergency is likely to be overblown. His justification for this is based on data for infection and fatality rates emerging from South Korea and Singapore that appear (currently) under control with only a relatively small proportion of their population infected. This was achieved without the country-wide lockdowns now being rolled out across Europe. Extrapolating from this experience, Richard suggests that the Coronavirus is not too contagious outside particular clusters of vulnerable individuals in situations like cruise ships and nursing homes.
The line of argument is vulnerable to the same criticism that one should never reason from a price change. The classic case of reasoning from a price change is reading oil prices as a measure of economic health. When oil prices drop, it could herald an economic boom or, paradoxically, a recession. If the price dropped because supply increased, when OPEC fails to enforce a price floor, then that lower price should stimulate the rest of the economy as transport and travel become cheaper. But if the price drops because economic activity is already dropping, and oil suppliers are struggling to sell at high prices, then the economy is heading towards a recession. The same measure can mean the opposite depending on the underlying mechanism.
The same logic applies to epidemics. The transmission rate is a combination of the (potentially changing) qualities of the virus and the social environment in which it spreads. The social environment is determined, among other things, by social distancing and tracking. Substantial changes in lifestyle can have initially marginal, but day after day very large, impacts on the infection rate. When combined with the medium-term fixed capacity of existing health systems, those rates translate into the difference between 50,000 and 500,000 deaths. You can’t look at relatively low fatality rates in some specific cases to project rates elsewhere without understanding what caused them to be the rate they are.
Right now, we don’t know for sure if the infection is controllable in the long run. However, we now know that South Korea and Singapore controlled the spread so far and also had systems in place to test, track and quarantine carriers of the virus. We also now know that Italy, without such a system, has been overrun with serious cases and a tragic increase in deaths. We know that China, having suppressed knowledge and interventions to contain the virus for several months, got the virus under control only through aggressive lockdowns.
So the case studies, for the moment, suggest social distancing and contact tracing can reduce cases if applied very early on. But more draconian measures are the only response if testing isn’t immediately available and contact tracing fails. Now is sadly not the time for half-measures or complacency.
I believe that Richard’s estimated fatality rates (less than 50,000 fatalities in the US) are ultimately plausible, but optimistic at this stage. Perversely, they are only plausible at all insofar as people project a much higher future fatality rate now. People must act with counter-intuitively strong measures before there is clear and obvious evidence it is needed. Like steering a large ship, temporally distant sources of danger must prompt radical action now. We will be lucky if we feel like we did too much in a few months’ time. Richard believes people are more worried than warranted right now. I think that’s exactly how worried people need to be to adopt the kind of adaptive behaviors that Richard relies on to explain how the spread of infection will stabilise.
Nightcap
- Our cities, our selves Jason Jewell, Modern Age
- Waiting for the wave to break Chris Bertram, Crooked Timber
- Midcentury life in the Soviet Union Alex Halberstadt, Literary Hub
- Britain’s colonial crimes and trade Jamil Anderlini, Financial Times
Human Capital Diversification vs Pancake Mix
I went to the grocery store yesterday (late morning) expecting either business-as-usual or empty shelves. I was surprised to see both. I’m currently regretting not taking photos because it probably will be business-as-usual by the time I go back.
Some shelves were empty, and others were full. What I saw was a direct visualization of what my neighbors don’t know how to cook.
Going through my store I could see that my neighbors know how to put jarred sauce on pasta. But I saw the opportunity to blend some canned whole tomatoes and make my own sauce. “International” foods were largely untouched, but anything in the local culinary lexicon was sparse.
The whole Baking Needs aisle was basically fine, except for the pancake mix which was all gone. This is really the whole story. Who buys pancake mix? Culinary illiterates.
(Disclaimer: I’m a biased source when it comes to pancakes. I take pancakes as seriously as 75th percentile Bostonian takes the fact that the Yankees suck.)
It takes a modest amount of skill to make pancakes, but the ingredients are cheap and YouTube wants to help you. Now is a great time to up your pancake game. But even if you just follow the directions on any random pancake recipe you’re stirring together flour, salt, baking powder, sugar, eggs, oil, and milk.
The mix will either give you a crappy shelf-stable replacement for the eggs and/or milk (yuck!) or hold your hand as you stir together some powder with eggs, oil, and milk.
Thinking back to my career as an omnivore, I can recall a time when I’ve bought ingredients I really should have made. I’m not judging people who don’t know how to cook, because I’ve been there.
What I’m pointing out is that those people are always going to have the hardest time when it comes to food shortages. I’d be in the same boat if I was shopping at a store that didn’t sell the limited set of ingredients I know how to use.
There’s a tension in economics that we don’t pay enough attention to: gains from specialization vs. gains from diversification. At a system level (and in a Principles class) the two go together. But at the level of individual there is a lot to be said for diversification–you’re more robust to change, resilient in the face of problems, and perspectives gained in one domain may have lessons to apply to others.
I’m grateful I haven’t taken my own human capital specialization so far that I can’t make my own pancakes.
